

A Robust Estimator of Malaria Incidence from Routine Health Facility Data
- PMID: 31833469
- PMCID: PMC7124910
- DOI: 10.4269/ajtmh.19-0600
A Robust Estimator of Malaria Incidence from Routine Health Facility Data
Abstract
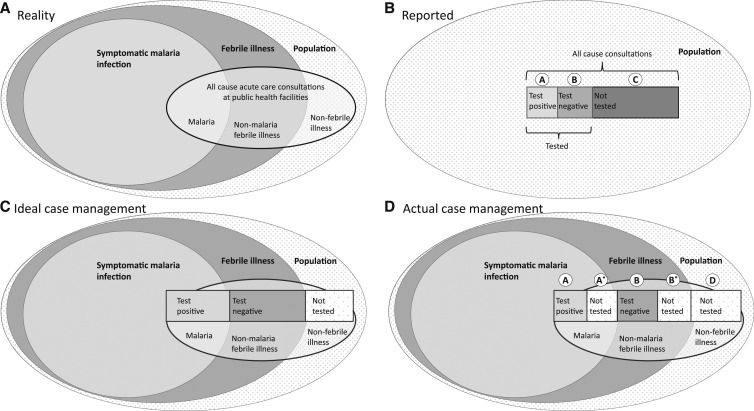
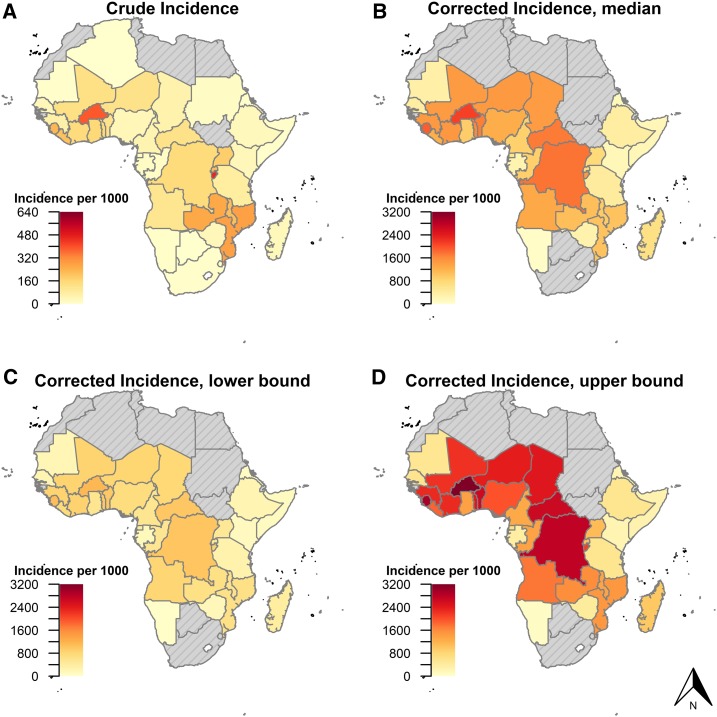
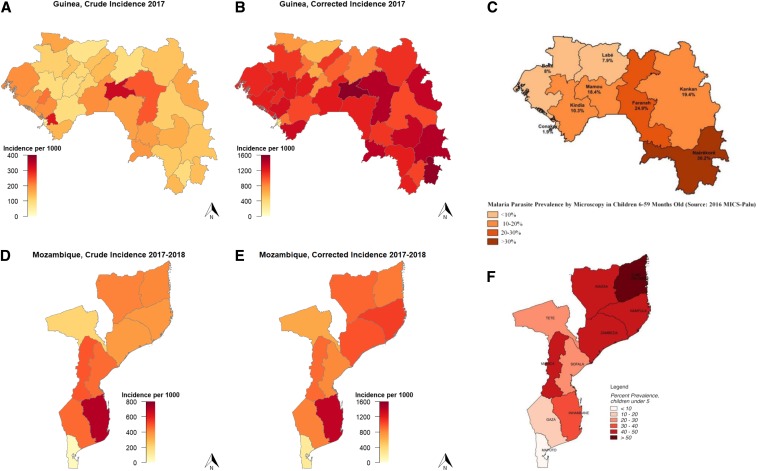
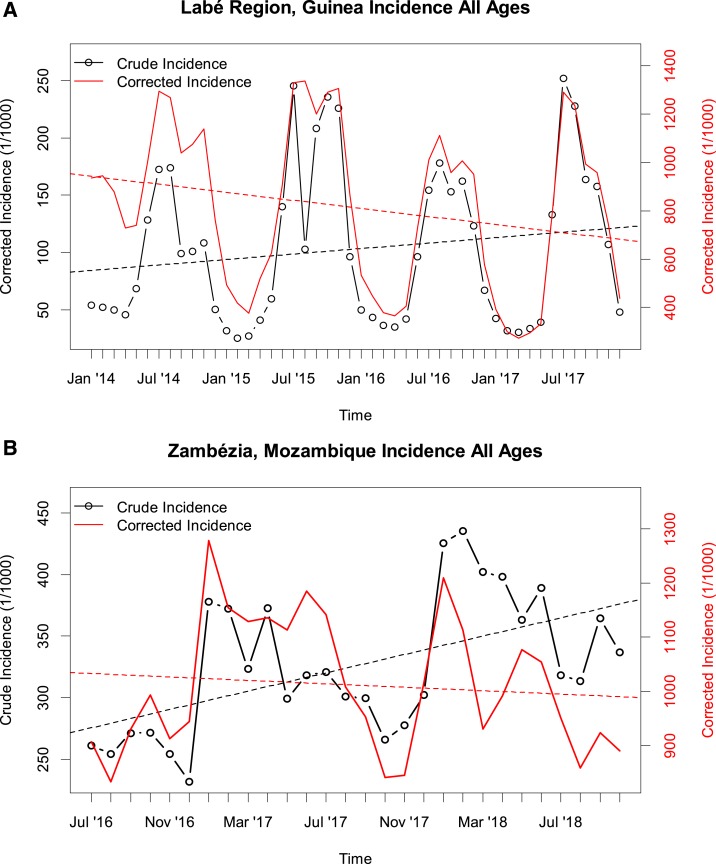
Routine incident malaria case data have become a pillar of malaria surveillance in sub-Saharan Africa. These data provide granular, timely information to track malaria burden. However, incidence data are sensitive to changes in care seeking rates, rates of testing of suspect cases, and reporting completeness. Based on a set of assumptions, we derived a simple algebraic formula to convert crude incidence rates to a corrected estimation of incidence, adjusting for biases in variable and suboptimal rates of care seeking, testing of suspect cases, and reporting completeness. We applied the correction to routine incidence data from Guinea and Mozambique, and aggregate data for sub-Saharan African countries from the World Malaria Report. We calculated continent-wide needs for malaria tests and treatments, assuming universal testing but current care seeking rates. Countries in southern and eastern Africa reporting recent increases in malaria incidence generally had lower overall corrected incidence than countries in Central and West Africa. Under current care seeking rates, the unmet need for malaria tests was estimated to be 160 million (M) (interquartile range [IQR]: 139-188) and for malaria treatments to be 37 M (IQR: 29-51). Maps of corrected incidence were more consistent with maps of community survey prevalence than was crude incidence in Guinea and Mozambique. Crude malaria incidence rates need to be interpreted in the context of suboptimal testing and care seeking rates, which vary over space and time. Adjusting for these factors can provide insight into the spatiotemporal trends of malaria burden.
Conflict of interest statement
Disclaimer: The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the CDC.
Disclosure: Excel tools for applying the robust estimator are freely available at
Figures
References
-
- World Health Organization , 2018. World Malaria Report 2018. Geneva, Switzerland: WHO.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
