

Does An Augmented Reality-based Portable Navigation System Improve the Accuracy of Acetabular Component Orientation During THA? A Randomized Controlled Trial
- PMID: 31834164
- PMCID: PMC7170692
- DOI: 10.1097/CORR.0000000000001083
Does An Augmented Reality-based Portable Navigation System Improve the Accuracy of Acetabular Component Orientation During THA? A Randomized Controlled Trial
Abstract
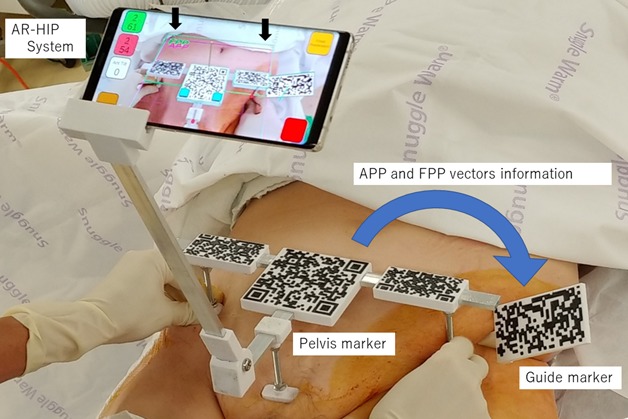
Background: We developed an augmented reality (AR)-based portable navigation system in which the surgeon can view the pelvic plane and placement angle of an acetabular cup on the display of a smartphone during THA.
Questions/purposes: (1) Is acetabular component placement more accurate using the AR-based portable navigation system compared with the conventional freehand technique? (2) Is intraoperative measurement of placement angle more accurate when using the AR-based portable navigation system compared with a goniometer?
Methods: Forty-six patients were randomly assigned to undergo acetabular cup placement during THA using the AR-based portable navigation system (AR navigation group) or placement of a mechanical alignment guide (conventional group). All surgeries were performed with the patient in the lateral decubitus position. We compared the absolute value of the difference between the targeted placement angle and postoperative measured placement angle between the groups using two types of imaging (radiography and CT).
Results: In terms of radiographic inclination, the mean differences between the targeted placement angle and postoperative measured angle were smaller in the AR navigation group than in the conventional group for both radiographs and CT images (2.3° ± 1.4° versus 3.9° ± 2.4°, respectively; p = 0.009 and 1.9° ± 1.3° versus 3.4° ± 2.6°, respectively; p = 0.02). There were no differences in radiographic anteversion between the two groups. No complications were associated with the use of the AR-based portable navigation system.
Conclusions: This system yielded no differences in acetabular anteversion accuracy, and no clinically important differences in acetabular inclination. Therefore, at this time we cannot recommend this device as its costs and risks cannot be justified based on the absence of a clinically meaningful difference in cup placement accuracy. Although we detected no complications, this was a small series, and this approach adds both surgical time and pins in the ilium.
Level of evidence: Level I, therapeutic study.
Conflict of interest statement
Each author certifies that neither he nor she, nor any member of his or her immediate family, has funding or commercial associations (e.g., consultancies, stock ownership, equity interest, patent/licensing arrangements) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and
Figures


 is the direction vector from R (right anterior superior iliac spine) to L (left anterior superior iliac spine). The vector
is the direction vector from R (right anterior superior iliac spine) to L (left anterior superior iliac spine). The vector  is the direction vector from R to P (pubic symphysis). The vector
is the direction vector from R to P (pubic symphysis). The vector  is the gravitational vector. The vector
is the gravitational vector. The vector  is defined as the normal vector of APP and is calculated with the cross product of
is defined as the normal vector of APP and is calculated with the cross product of  and
and  . The vector
. The vector  is defined as the cross product of
is defined as the cross product of  and
and  and it is perpendicular to both
and it is perpendicular to both  and
and  . The vector
. The vector  is defined as the normal vector of FPP and is calculated with the cross product of
is defined as the normal vector of FPP and is calculated with the cross product of  and
and  .
.

 is the direction vector of the cup handle. The angle of radiographic anteversion is calculated with the inner product of
is the direction vector of the cup handle. The angle of radiographic anteversion is calculated with the inner product of  and
and  . The angle of radiographic inclination is calculated with the cross product of
. The angle of radiographic inclination is calculated with the cross product of  and
and  and the inner product of
and the inner product of  and this cross product.
and this cross product.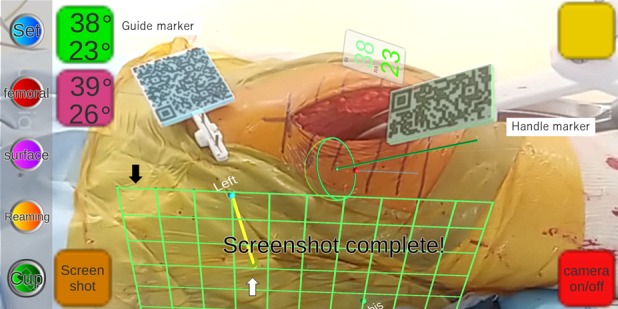


Comment in
-
Editor's Spotlight/Take 5: Does An Augmented Reality-based Portable Navigation System Improve the Accuracy of Acetabular Component Orientation During THA? A Randomized Controlled Trial.Clin Orthop Relat Res. 2020 May;478(5):931-934. doi: 10.1097/CORR.0000000000001216. Clin Orthop Relat Res. 2020. PMID: 32168058 Free PMC article. No abstract available.
References
-
- Ankita G, Kriti B, Kritika G, Manu V. Comparative study of marker-based and marker-less indoor navigation in augmented reality. International Research Journal of Engineering and Technology. 2018;5:3569-3572.
-
- Bohl DD, Nolte MT, Ong K, Lau E, Calkins TE, Della Valle CJ. Computer-Assisted Navigation Is Associated with Reductions in the Rates of Dislocation and Acetabular Component Revision Following Primary Total Hip Arthroplasty. J Bone Joint Surg Am . 2019;101(3):250-256. - PubMed
-
- Christopher R, Blake E, Julia R, James L, Brett D. The use of fluoroscopy during direct anterior hip arthroplasty: powerful or misleading? J Arthroplasty . 2018;33:1775-1779. - PubMed
-
- D'Lima DD, Urquhart AG, Buehler KO, Walker RH, Colwell CW., Jr The effect of the orientation of the acetabular and femoral components on the range of motion of the hip at different head-neck ratios. J Bone Joint Surg Am. 2000;82:315-321. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
