

Assessment of the Cost-Effectiveness of a Brief Video Intervention for Sexually Transmitted Disease Prevention
- PMID: 31834206
- PMCID: PMC7590367
- DOI: 10.1097/OLQ.0000000000001109
Assessment of the Cost-Effectiveness of a Brief Video Intervention for Sexually Transmitted Disease Prevention
Erratum in
-
Erratum - Assessment of the Cost-Effectiveness of a Brief Video Intervention for Sexually Transmitted Disease Prevention.Sex Transm Dis. 2020 Apr;47(4):e9. doi: 10.1097/OLQ.0000000000001136. Sex Transm Dis. 2020. PMID: 32044863 No abstract available.
Abstract
Background: Cost-effective, scalable interventions are needed to address high rates of sexually transmitted diseases (STDs) in the United States. Safe in the City, a 23-minute video intervention designed for STD clinic waiting rooms, effectively reduced new infections among STD clinic clients. A cost-effectiveness analysis of this type of intervention could inform whether it should be replicated.
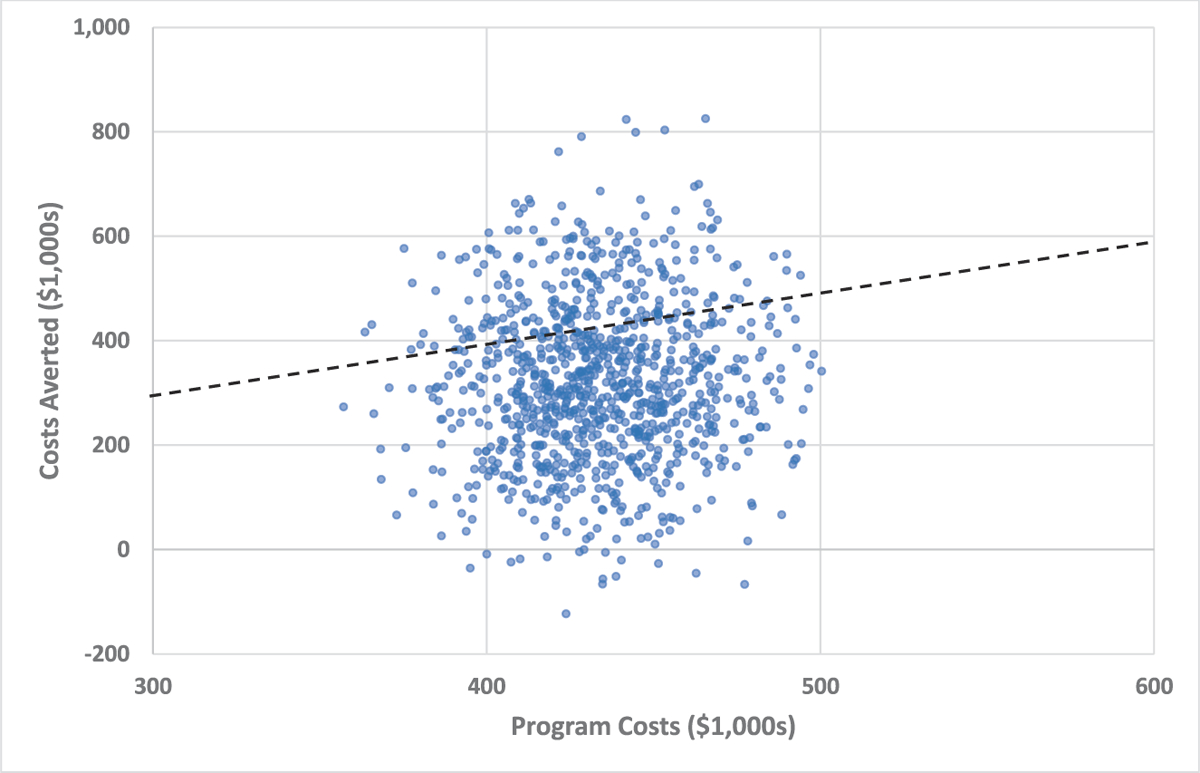
Methods: The cost-effectiveness of a brief video intervention was calculated under a baseline scenario in which this type of intervention was expanded to a larger patient population. Alternative scenarios included expanding the intervention over a longer period or to more clinics, including HIV prevention benefits, and operating the intervention part time. Program costs, net costs per STD case averted, and the discounted net cost of the intervention were calculated from a health sector perspective across the scenarios. Monte Carlo simulations were used to calculate 95% confidence intervals surrounding the cost-effectiveness measures.
Results: The net cost per case averted was $75 in the baseline scenario. The net cost of the intervention was $108,015, and most of the alternative scenarios found that the intervention was cost saving compared with usual care.
Conclusions: Single session, video-based interventions can be highly cost effective when implemented at scale. Updated video-based interventions that account for the changing STD landscape in the United States could play an important role in addressing the recent increases in infections.
Conflict of interest statement
Conflict of Interest and Sources of Funding: None declared.
Figures
References
-
- Satterwhite CL, Torrone E, Meites E, et al. Sexually transmitted infections among US women and men: Prevalence and incidence estimates, 2008. Sex Transm Dis 2013; 40:187–193. - PubMed
-
- Owusu-Edusei K Jr., Chesson H, Gift TL, et al. The estimated direct medical cost of selected sexually transmitted infections in the United States, 2008. Sex Transm Dis 2013; 40:197–201. - PubMed
-
- Myint-U A, Bull S, Greenwood GL, et al. Safe in the City: Developing an effective video-based intervention for STD clinic waiting rooms. Health Promot Pract 2010; 11:408–417. - PubMed
-
- Harshbarger CL, O’Donnell LN, Warner L, et al. Safe in the City: Effective prevention interventions for human immunodeficiency virus and sexually transmitted infections. Am J Prev Med 2012; 42:468–472. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
