

Intercostal nerve block of the anterior cutaneous branches and the sensibility of the female breast
- PMID: 31837172
- PMCID: PMC7540051
- DOI: 10.1002/ca.23532
Intercostal nerve block of the anterior cutaneous branches and the sensibility of the female breast
Abstract
Introduction: Better sensation in the reconstructed breast improves the quality of life. Sensory nerve coaptation is a valuable addition to autologous breast reconstruction. There are few publications concerning the sensory nerves of the breast and the nipple-areola complex and reports are contradictory, so it is unknown which nerve is best suited as a recipient for coaptation. The current study serves as a proof of concept.
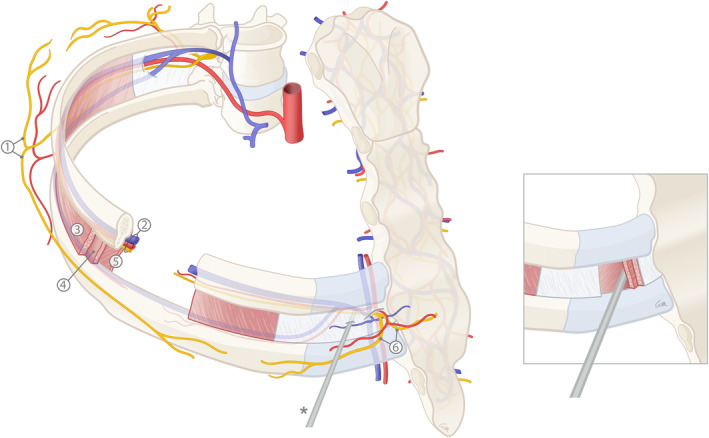
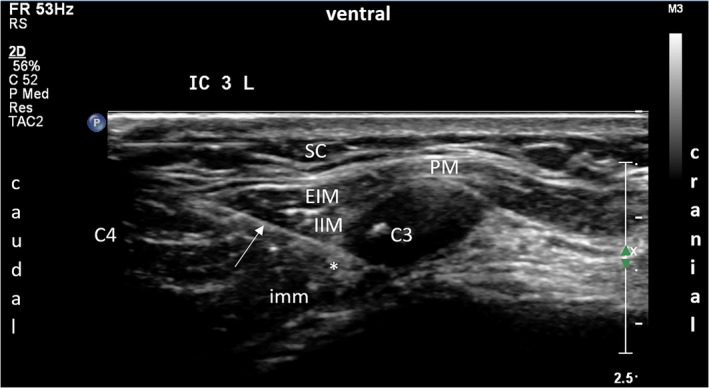
Materials and methods: The areas innervated by the anterior cutaneous branches (ACBs) of the intercostal nerves (ICNs) were studied on two separate occasions in two healthy women. First, the ACBs of ICNs 2-5 were individually blocked using ultrasound. Next, the ACBs of all levels were blocked simultaneously. Sensation was measured using Semmes-Weinstein monofilaments. The numbed areas corresponding to the ICNs were drawn in a raster of 2 × 2 cm.
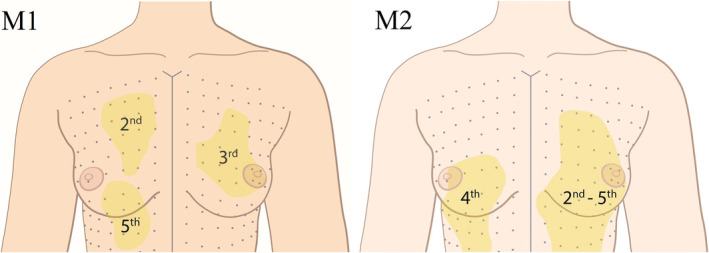
Results: The largest area was supplied by the ACB of the 4th ICN, located in the upper (UIQ) and the lower (LIQ) inner quadrants of the breast. The 2nd-largest area was supplied by the ACB of the 3rd ICN. Blockage of ACBs 2-5 affected sensation in the nipple and the areola.
Conclusions: Blockage of all levels 2-5 partially affected sensation in the nipple-areola complex, suggesting innervation by a nerve plexus consisting of both ACBs and lateral cutaneous branches (LCBs). ACB4 supplied the largest area of the breast in the UIQ and LIQ and could be best suited for sensory nerve coaptation to optimize sensation in the autologously reconstructed breast.
Keywords: breast cancer; breast reconstruction; intercostal nerve; nipple-areola complex; sensation.
© 2019 The Authors. Clinical Anatomy published by Wiley Periodicals, Inc. on behalf of American Association of Clinical Anatomists.
Conflict of interest statement
The authors state that they have no conflict of interest.
Figures


References
-
- Beugels, J. , Cornelissen, A. J. M. , van Kuijk, S. M. J. , Lataster, A. , Heuts, E. M. , Piatkowski, A. , … Tuinder, S. M. H. (2019). Sensory recovery of the breast following innervated and noninnervated DIEP flap breast reconstruction. Plastic and Reconstructive Surgery, 144, 178e–188e. - PubMed
-
- Cooper, A. (1840). The anatomy of the breast. London: Longman.
-
- Craig, R. D. , & Sykes, P. A. (1970). Nipple sensitivity following reduction mammaplasty. British Journal of Plastic Surgery, 23, 165–172. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
