

Delirium is prevalent in older hospital inpatients and associated with adverse outcomes: results of a prospective multi-centre study on World Delirium Awareness Day
- PMID: 31837711
- PMCID: PMC6911703
- DOI: 10.1186/s12916-019-1458-7
Delirium is prevalent in older hospital inpatients and associated with adverse outcomes: results of a prospective multi-centre study on World Delirium Awareness Day
Abstract
Background: Delirium is a common severe neuropsychiatric condition secondary to physical illness, which predominantly affects older adults in hospital. Prior to this study, the UK point prevalence of delirium was unknown. We set out to ascertain the point prevalence of delirium across UK hospitals and how this relates to adverse outcomes.
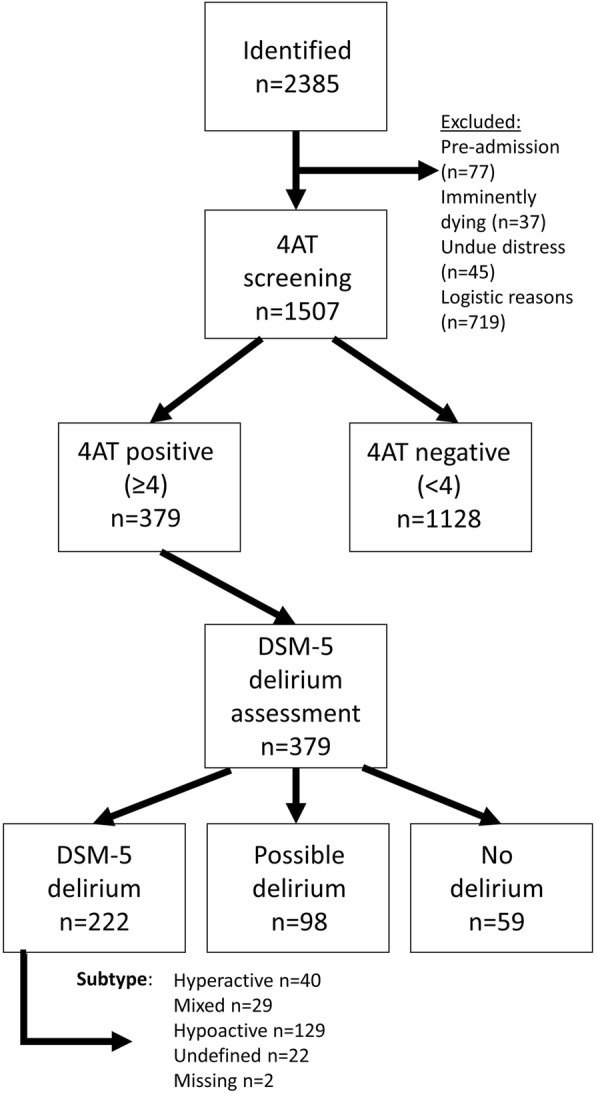
Methods: We conducted a prospective observational study across 45 UK acute care hospitals. Older adults aged 65 years and older were screened and assessed for evidence of delirium on World Delirium Awareness Day (14th March 2018). We included patients admitted within the previous 48 h, excluding critical care admissions.
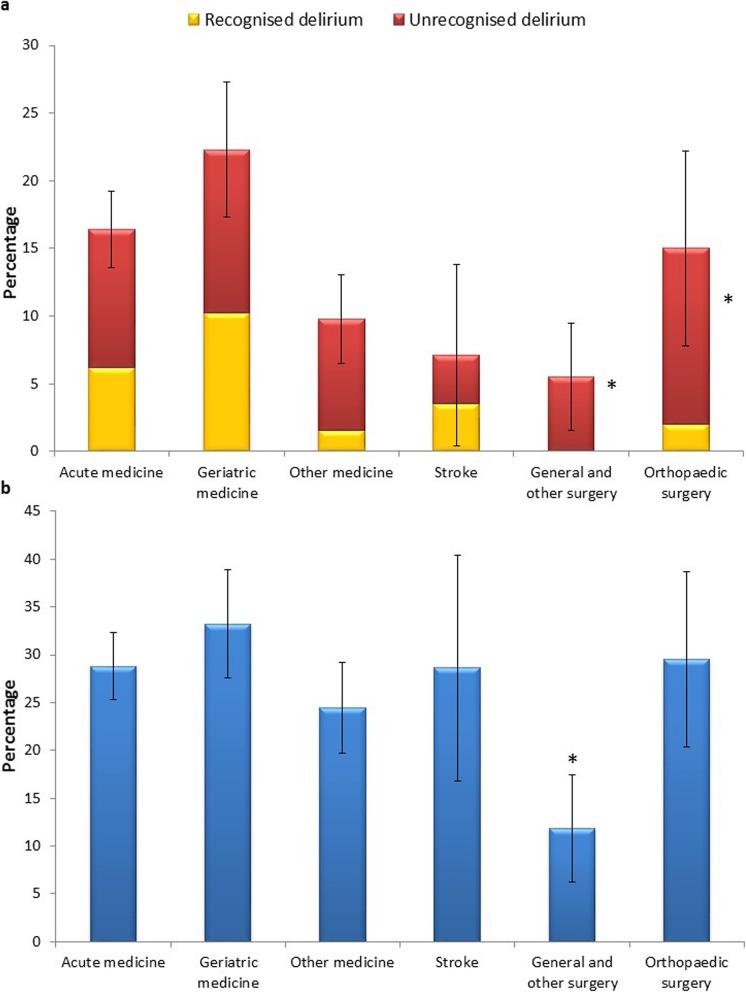
Results: The point prevalence of Diagnostic and Statistical Manual on Mental Disorders, Fifth Edition (DSM-5) delirium diagnosis was 14.7% (222/1507). Delirium presence was associated with higher Clinical Frailty Scale (CFS): CFS 4-6 (frail) (OR 4.80, CI 2.63-8.74), 7-9 (very frail) (OR 9.33, CI 4.79-18.17), compared to 1-3 (fit). However, higher CFS was associated with reduced delirium recognition (7-9 compared to 1-3; OR 0.16, CI 0.04-0.77). In multivariable analyses, delirium was associated with increased length of stay (+ 3.45 days, CI 1.75-5.07) and increased mortality (OR 2.43, CI 1.44-4.09) at 1 month. Screening for delirium was associated with an increased chance of recognition (OR 5.47, CI 2.67-11.21).
Conclusions: Delirium is prevalent in older adults in UK hospitals but remains under-recognised. Frailty is strongly associated with the development of delirium, but delirium is less likely to be recognised in frail patients. The presence of delirium is associated with increased mortality and length of stay at one month. A national programme to increase screening has the potential to improve recognition.
Keywords: Collaboration; Delirium; Frailty; Older adults.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders (DSM-5®) 5 2013.
-
- Ryan Daniel James, O'Regan Niamh Annmarie, Caoimh Ronán Ó, Clare Josie, O'Connor Marie, Leonard Maeve, McFarland John, Tighe Sheila, O'Sullivan Kathleen, Trzepacz Paula T, Meagher David, Timmons Suzanne. Delirium in an adult acute hospital population: predictors, prevalence and detection. BMJ Open. 2013;3(1):e001772. doi: 10.1136/bmjopen-2012-001772. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
