

Diuretic Strategies for Loop Diuretic Resistance in Acute Heart Failure: The 3T Trial
- PMID: 31838029
- PMCID: PMC7058489
- DOI: 10.1016/j.jchf.2019.09.012
Diuretic Strategies for Loop Diuretic Resistance in Acute Heart Failure: The 3T Trial
Abstract
Objectives: This study compared combination diuretic strategies in acute heart failure (AHF) complicated by diuretic resistance (DR).
Background: Combination diuretic regimens to overcome loop DR are commonly used but with limited evidence.
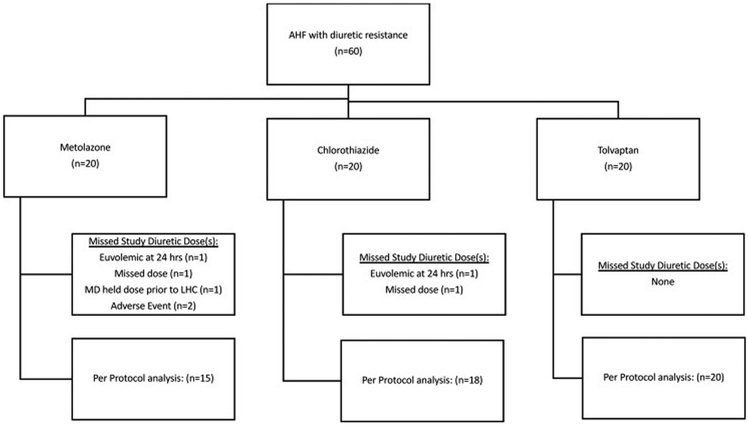
Methods: This study was a randomized, double-blinded trial in 60 patients hospitalized with AHF and intravenous (IV) loop DR. Patients were randomized to oral metolazone, IV chlorothiazide, or tolvaptan therapy. All patients received concomitant high-dose IV infusions of furosemide. The primary outcome was 48-h weight loss.
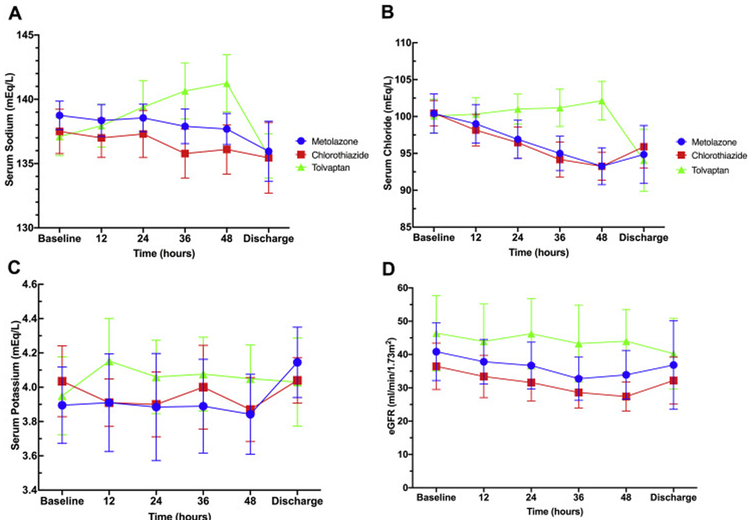
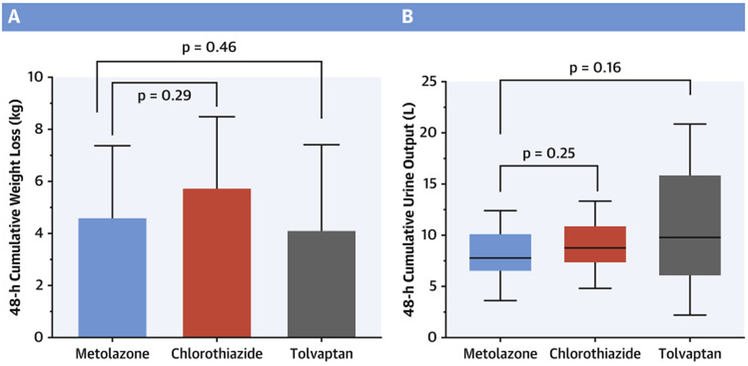
Results: The cohort exhibited DR prior to enrollment, producing 1,188 ± 476 ml of urine in 12 h during high-dose loop diuretic therapy (IV furosemide: 612 ± 439 mg/day). All 3 interventions significantly improved diuretic efficacy (p < 0.001). Compared to metolazone (4.6 ± 2.7 kg), neither IV chlorothiazide (5.8 ± 2.7 kg; 1.2 kg [95% confidence interval (CI)]: -2.9 to 0.6; p = 0.292) nor tolvaptan (4.1 ± 3.3 kg; 0.5 kg [95% CI: -1.5 to 2.4; p = 0.456) resulted in more weight loss at 48 h. Median (interquartile range [IQR]) cumulative urine output increased significantly and did not differ among those receiving metolazone (7.78 [IQR: 6.59 to 10.10] l) and chlorothiazide (8.77 [IQR: 7.37 to 10.86] l; p = 0.245) or tolvaptan (9.70 [IQR: 6.36 to 13.81] l; p = 0.160). Serum sodium decreased less with tolvaptan than with metolazone (+4 ± 5 vs. -1 ± 3 mEq/l; p = 0.001), but 48-h spot urine sodium was lower with tolvaptan (58 ± 25 mmol/l) than with metolazone (104 ± 16 mmol/l; p = 0.002) and with chlorothiazide (117 ± 14 mmol/l; p < 0.001).
Conclusions: In this moderately sized DR trial, weight loss was excellent with the addition of metolazone, IV chlorothiazide, or tolvaptan to loop diuretics, without a detectable between-group difference. (Comparison of Oral or Intravenous Thiazides vs. tolvaptan in Diuretic Resistant Decompensated Heart Failure [3T]; NCT02606253).
Keywords: acute heart failure; diuretic resistance; diuretics; heart failure; thiazide; tolvaptan.
Copyright © 2020 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Is Resistance Futile?: Addressing Diuretic Resistance During Hospitalization for Heart Failure.JACC Heart Fail. 2020 Mar;8(3):169-171. doi: 10.1016/j.jchf.2019.10.008. Epub 2020 Jan 8. JACC Heart Fail. 2020. PMID: 31926852 No abstract available.
References
-
- Yancy CW, Jessup M, Bozkurt B et al. 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Journal of the American College of Cardiology 2013;62:1495–1539. - PubMed
-
- Ponikowski P, Voors AA, Anker SD et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. European heart journal 2016;37:2129–2200. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
