

Distinct Polygenic Score Profiles in Schizophrenia Subgroups With Different Trajectories of Cognitive Development
- PMID: 31838871
- PMCID: PMC9627722
- DOI: 10.1176/appi.ajp.2019.19050527
Distinct Polygenic Score Profiles in Schizophrenia Subgroups With Different Trajectories of Cognitive Development
Abstract
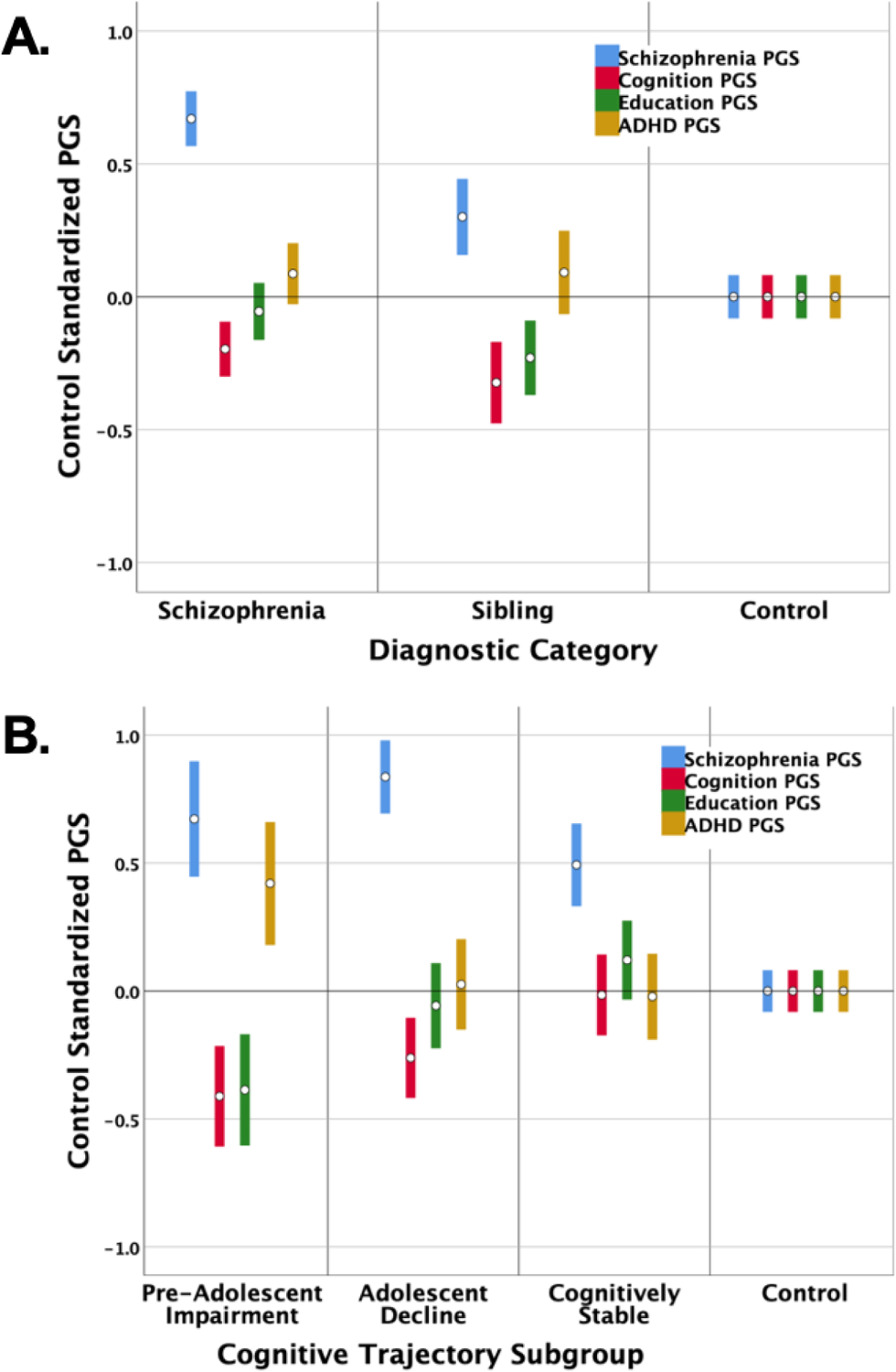
Objective: Different cognitive development histories in schizophrenia may reflect variation across dimensions of genetic influence. The authors derived and characterized cognitive development trajectory subgroups within a schizophrenia sample and profiled the subgroups across polygenic scores (PGSs) for schizophrenia, cognition, educational attainment, and attention deficit hyperactivity disorder (ADHD).
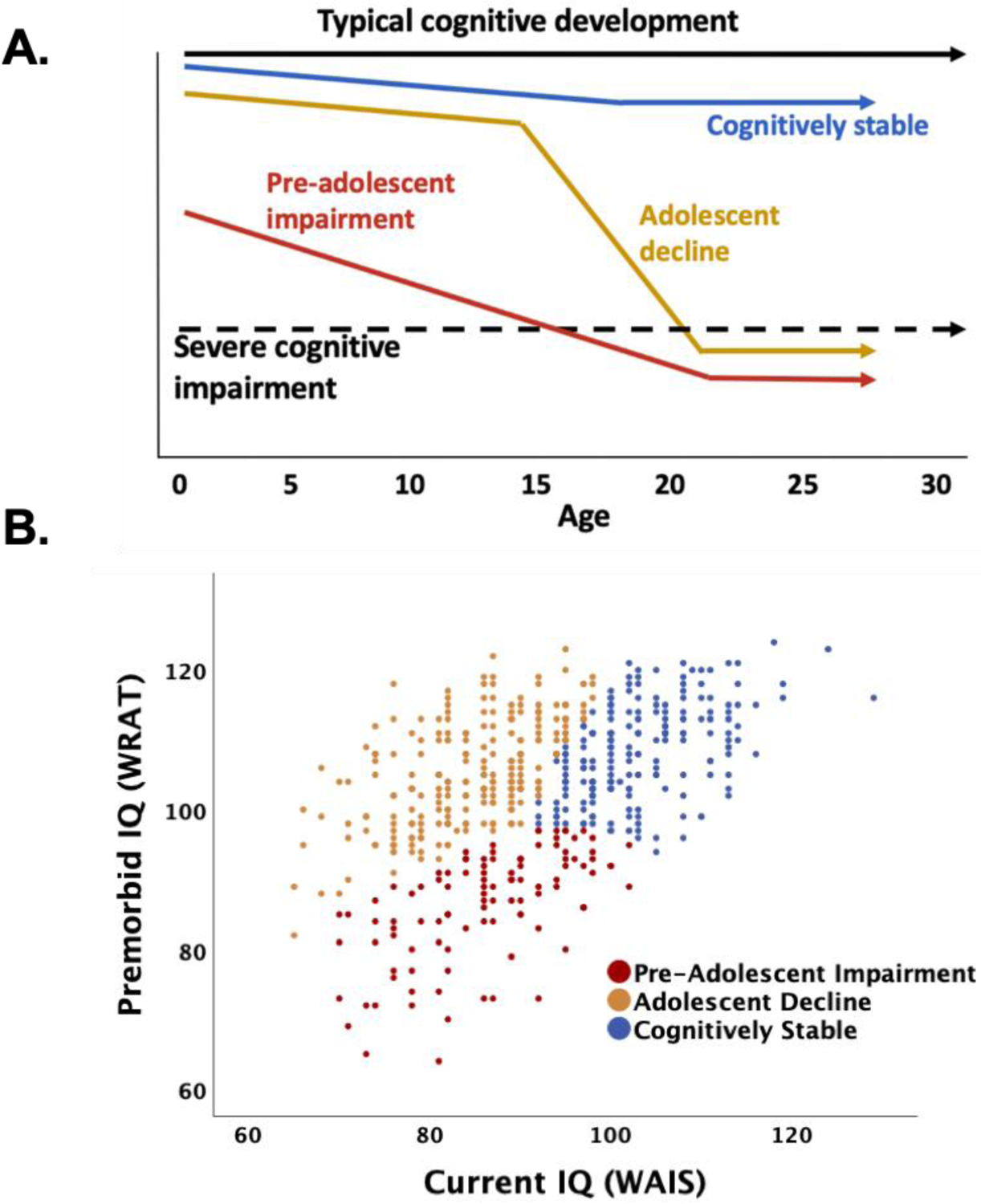
Methods: Demographic, clinical, and genetic data were collected at the National Institute of Mental Health from 540 schizophrenia patients, 247 unaffected siblings, and 844 control subjects. Cognitive trajectory subgroups were derived through cluster analysis using estimates of premorbid and current IQ. PGSs were generated using standard methods. Associations were tested using general linear models and logistic regression.
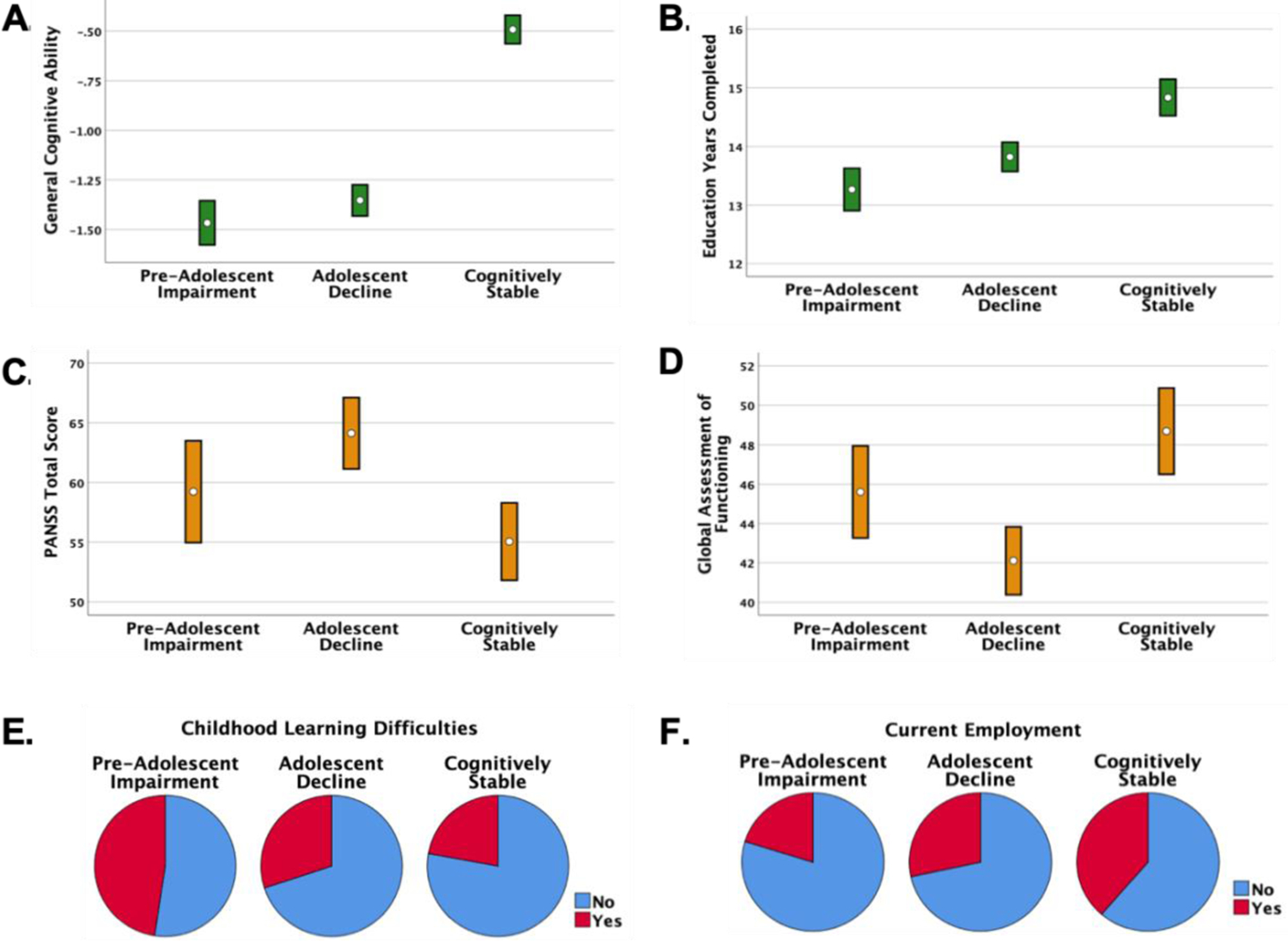
Results: Cluster analyses identified three cognitive trajectory subgroups in the schizophrenia group: preadolescent cognitive impairment (19%), adolescent disruption of cognitive development (44%), and cognitively stable adolescent development (37%). Together, the four PGSs significantly predicted 7.9% of the variance in subgroup membership. Subgroup characteristics converged with genetic patterns. Cognitively stable individuals had the best adult clinical outcomes and differed from control subjects only in schizophrenia PGSs. Those with adolescent disruption of cognitive development showed the most severe symptoms after diagnosis and were cognitively impaired. This subgroup had the highest schizophrenia PGSs and had disadvantageous cognitive PGSs relative to control subjects and cognitively stable individuals. Individuals showing preadolescent impairment in cognitive and academic performance and poor adult outcome exhibited a generalized PGS disadvantage relative to control subjects and were the only subgroup to differ significantly in education and ADHD PGSs.
Conclusions: Subgroups derived from patterns of premorbid and current IQ showed different premorbid and clinical characteristics, which converged with broad genetic profiles. Simultaneous analysis of multiple PGSs may contribute to useful clinical stratification in schizophrenia.
Keywords: Cognition; Developmental Trajectory; Genetics; Polygenic Score; Premorbid IQ; Schizophrenia.
Conflict of interest statement
The authors report no financial relationships with relevant commercial interests.
Figures
Comment in
-
Genetically, Developmentally, and Clinically Distinct Cognitive Subtypes in Schizophrenia: A Tale of Three Trajectories.Am J Psychiatry. 2020 Apr 1;177(4):282-284. doi: 10.1176/appi.ajp.2020.20020132. Am J Psychiatry. 2020. PMID: 32233679 No abstract available.
References
-
- Walker EF: Schizophrenia: A life-course developmental perspective. San Diego, CA, Academic Press, Inc.; 1991.
-
- Weinberger DR. Thinking About Schizophrenia in an Era of Genomic Medicine. Am J Psychiatry. 2019;176:12–20. - PubMed
-
- Mollon J, Reichenberg A. Cognitive development prior to onset of psychosis. Psychological Medicine. 2018;48:392–403. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
