

Use of anastrozole for breast cancer prevention (IBIS-II): long-term results of a randomised controlled trial
- PMID: 31839281
- PMCID: PMC6961114
- DOI: 10.1016/S0140-6736(19)32955-1
Use of anastrozole for breast cancer prevention (IBIS-II): long-term results of a randomised controlled trial
Erratum in
-
Department of Error.Lancet. 2020 Feb 15;395(10223):496. doi: 10.1016/S0140-6736(20)30323-8. Lancet. 2020. PMID: 32061297 Free PMC article. No abstract available.
-
Department of Error.Lancet. 2021 Feb 27;397(10276):796. doi: 10.1016/S0140-6736(21)00427-X. Lancet. 2021. PMID: 33640066 Free PMC article. No abstract available.
Abstract
Background: Two large clinical trials have shown a reduced rate of breast cancer development in high-risk women in the initial 5 years of follow-up after use of aromatase inhibitors (MAP.3 and International Breast Cancer Intervention Study II [IBIS-II]). Here, we report blinded long-term follow-up results for the IBIS-II trial, which compared anastrozole with placebo, with the objective of determining the efficacy of anastrozole for preventing breast cancer (both invasive and ductal carcinoma in situ) in the post-treatment period.
Methods: IBIS-II is an international, randomised, double-blind, placebo-controlled trial. Postmenopausal women at increased risk of developing breast cancer were recruited and were randomly assigned (1:1) to either anastrozole (1 mg per day, oral) or matching placebo daily for 5 years. After treatment completion, women were followed on a yearly basis to collect data on breast cancer incidence, death, other cancers, and major adverse events (cardiovascular events and fractures). The primary outcome was all breast cancer.
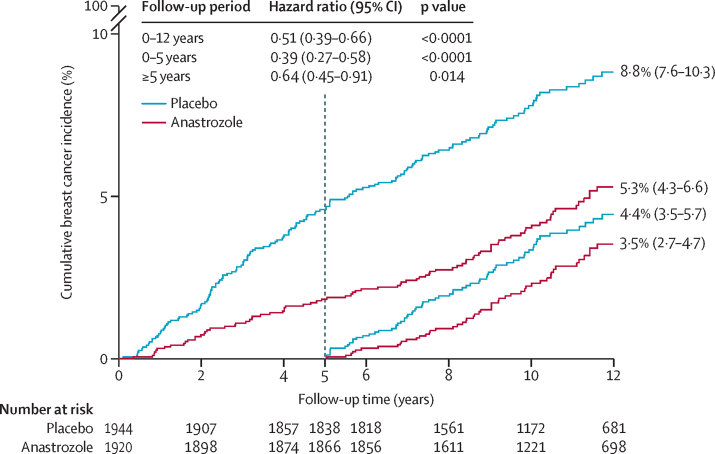
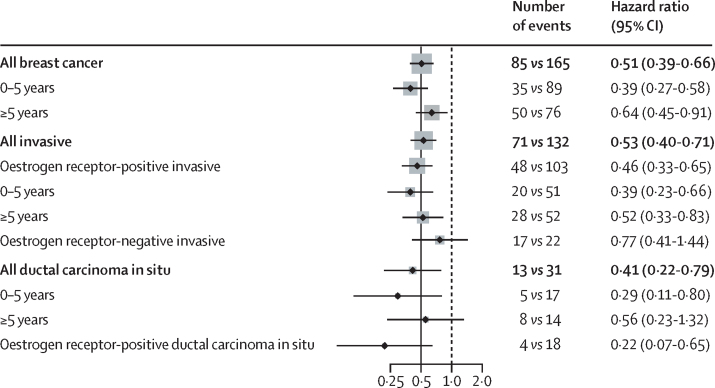
Findings: 3864 women were recruited between Feb 2, 2003, and Jan 31, 2012. 1920 women were randomly assigned to 5 years anastrozole and 1944 to placebo. After a median follow-up of 131 months (IQR 105-156), a 49% reduction in breast cancer was observed for anastrozole (85 vs 165 cases, hazard ratio [HR] 0·51, 95% CI 0·39-0·66, p<0·0001). The reduction was larger in the first 5 years (35 vs 89, 0·39, 0·27-0·58, p<0·0001), but still significant after 5 years (50 vs 76 new cases, 0·64, 0·45-0·91, p=0·014), and not significantly different from the first 5 years (p=0·087). Invasive oestrogen receptor-positive breast cancer was reduced by 54% (HR 0·46, 95% CI 0·33-0·65, p<0·0001), with a continued significant effect in the period after treatment. A 59% reduction in ductal carcinoma in situ was observed (0·41, 0·22-0·79, p=0·0081), especially in participants known to be oestrogen receptor-positive (0·22, 0·78-0·65, p<0·0001). No significant difference in deaths was observed overall (69 vs 70, HR 0·96, 95% CI 0·69-1·34, p=0·82) or for breast cancer (two anastrozole vs three placebo). A significant decrease in non-breast cancers was observed for anastrozole (147 vs 200, odds ratio 0·72, 95% CI 0·57-0·91, p=0·0042), owing primarily to non-melanoma skin cancer. No excess of fractures or cardiovascular disease was observed.
Interpretation: This analysis has identified a significant continuing reduction in breast cancer with anastrozole in the post-treatment follow-up period, with no evidence of new late side-effects. Further follow-up is needed to assess the effect on breast cancer mortality.
Funding: Cancer Research UK, the National Health and Medical Research Council Australia, Breast Cancer Research Foundation, Sanofi Aventis, and AstraZeneca.
Copyright © 2020 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Carryover effects of aromatase inhibitors in prevention.Lancet. 2020 Jan 11;395(10218):91-92. doi: 10.1016/S0140-6736(19)33102-2. Epub 2019 Dec 13. Lancet. 2020. PMID: 31843210 No abstract available.
-
In high-risk, postmenopausal women, 5 years of anastrozole reduced breast cancer incidence at 11 years.Ann Intern Med. 2020 Apr 21;172(8):JC45. doi: 10.7326/ACPJ202004210-045. Ann Intern Med. 2020. PMID: 32311729 No abstract available.
References
-
- Cuzick J, Sestak I, Forbes JF. Anastrozole for prevention of breast cancer in high-risk postmenopausal women (IBIS-II): an international, double-blind, randomised placebo-controlled trial. Lancet. 2014;383:1041–1048. - PubMed
-
- Goss PE, Ingle JN, Ales-Martinez JE. Exemestane for breast-cancer prevention in postmenopausal women. N Engl J Med. 2011;364:2381–2391. - PubMed
-
- Cuzick J, Sestak I, Baum M. Effect of anastrozole and tamoxifen as adjuvant treatment for early-stage breast cancer: 10-year analysis of the ATAC trial. Lancet Oncol. 2010;11:1135–1141. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
