

Unbound Plasma, Total Plasma, and Whole-Blood Tacrolimus Pharmacokinetics Early After Thoracic Organ Transplantation
- PMID: 31840222
- PMCID: PMC7292814
- DOI: 10.1007/s40262-019-00854-1
Unbound Plasma, Total Plasma, and Whole-Blood Tacrolimus Pharmacokinetics Early After Thoracic Organ Transplantation
Erratum in
-
Correction to: Unbound Plasma, Total Plasma and Whole-Blood Tacrolimus Pharmacokinetics Early After Thoracic Organ Transplantation.Clin Pharmacokinet. 2022 Apr;61(4):589. doi: 10.1007/s40262-022-01115-4. Clin Pharmacokinet. 2022. PMID: 35233710 Free PMC article. No abstract available.
Abstract
Background and objective: Therapeutic drug monitoring of tacrolimus whole-blood concentrations is standard care in thoracic organ transplantation. Nevertheless, toxicity may appear with alleged therapeutic concentrations possibly related to variability in unbound concentrations. However, pharmacokinetic data on unbound concentrations are not available. The objective of this study was to quantify the pharmacokinetics of whole-blood, total, and unbound plasma tacrolimus in patients early after heart and lung transplantation.
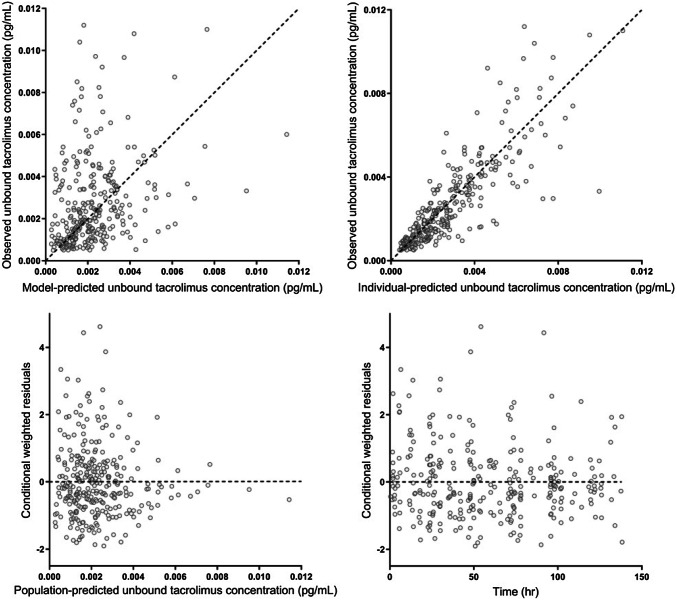
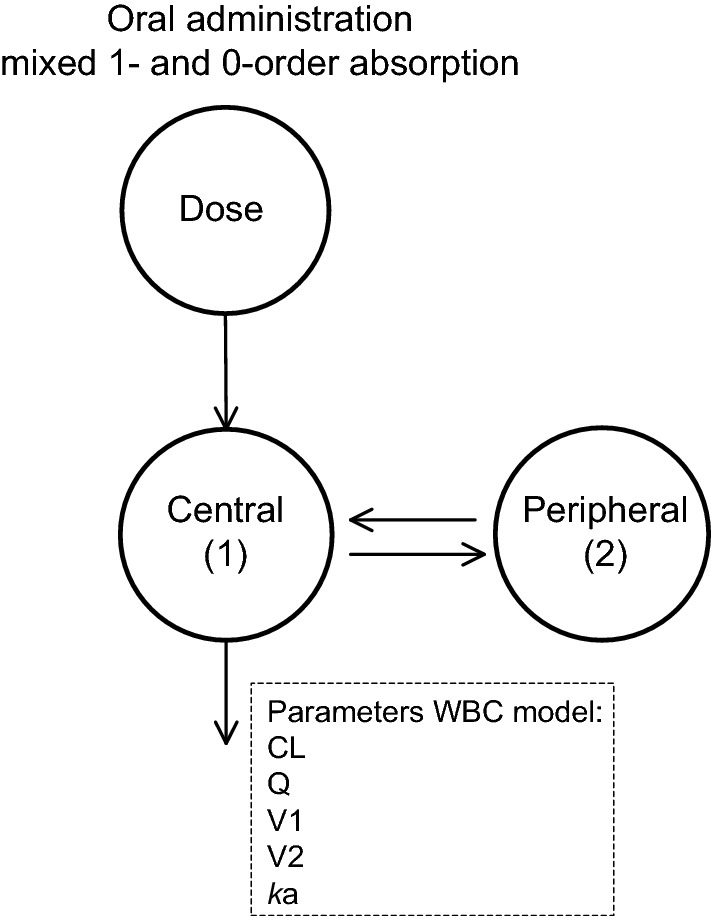
Methods: Twelve-hour tacrolimus whole-blood, total, and unbound plasma concentrations of 30 thoracic organ recipients were analyzed with high-performance liquid chromatography-tandem mass spectrometry directly after transplantation. Pharmacokinetic modeling was performed using non-linear mixed-effects modeling.
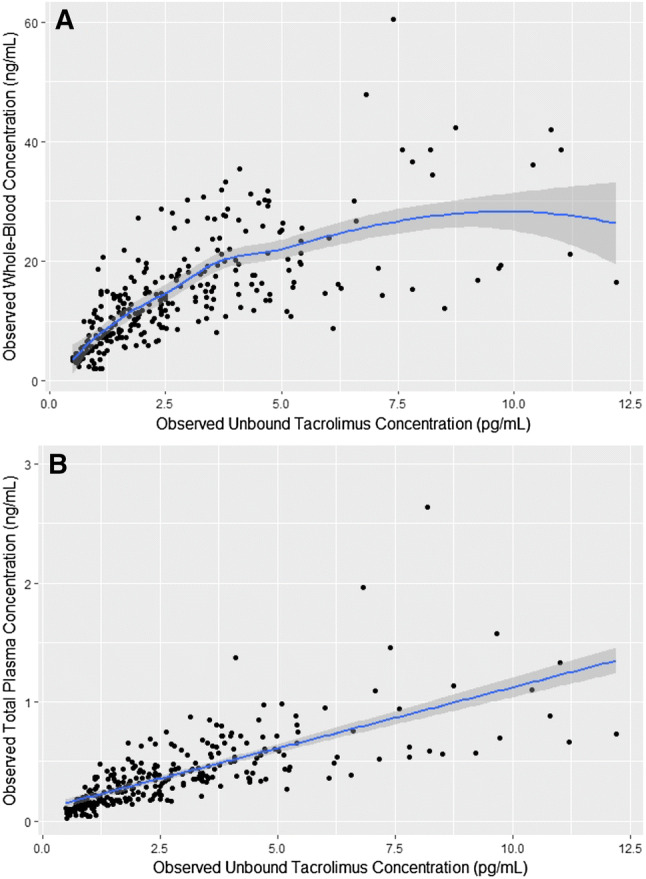
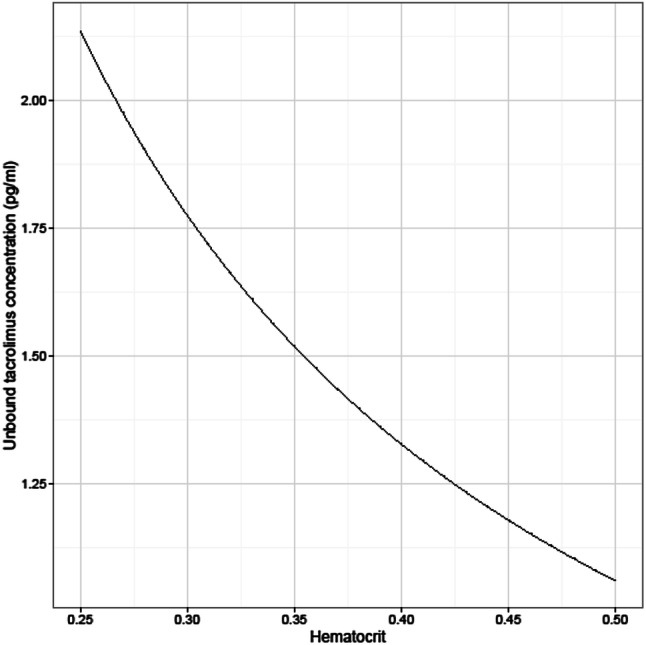
Results: Plasma concentration was < 1% of the whole-blood concentration. Maximum binding capacity of erythrocytes was directly proportional to hematocrit and estimated at 2700 pg/mL (95% confidence interval 1750-3835) with a dissociation constant of 0.142 pg/mL (95% confidence interval 0.087-0.195). The inter-individual variability in the binding constants was considerable (27% maximum binding capacity, and 29% for the linear binding constant of plasma).
Conclusions: Tacrolimus association with erythrocytes was high and suggested a non-linear distribution at high concentrations. Monitoring hematocrit-corrected whole-blood tacrolimus concentrations might improve clinical outcomes in clinically unstable thoracic organ transplants.
Clinical trial registration: NTR 3912/EudraCT 2012-001909-24.
Conflict of interest statement
Jozef Kesecioglu reports personal fees from an honorarium received from Xenios AG, outside the submitted work. Maaike A. Sikma, Erik M. Van Maarseveen, Claudine C. Hunault, Javier M. Moreno, Ed A. Van de Graaf, Johannes H. Kirkels, Marianne C. Verhaar, Jan C. Grutters, Dylan W. De Lange, and Alwin D.R. Huitema have no conflicts of interest that are directly relevant to the content of this study.
Figures
References
-
- Rayar M, Tron C, Jézéquel C, Beaurepaire J-M, Petitcollin A, Houssel-Debry P, et al. High intrapatient variability of tacrolimus exposure in the early period after liver transplantation is associated with poorer outcomes. Transplantation. 2018;102:e108–e114. doi: 10.1097/tp.0000000000002052. - DOI - PubMed
-
- Bouamar R, Shuker N, Hesselink DA, Weimar W, Ekberg H, Kaplan B, et al. Tacrolimus predose concentrations do not predict the risk of acute rejection after renal transplantation: a pooled analysis from three randomized-controlled clinical trials(†) Am J Transplant. 2013;13:1253–1261. doi: 10.1111/ajt.12191. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
