

Impact of a multidisciplinary quality improvement initiative to reduce inappropriate usage of stress ulcer prophylaxis in hospitalized patients
- PMID: 31840265
- PMCID: PMC7163370
- DOI: 10.1111/bcp.14197
Impact of a multidisciplinary quality improvement initiative to reduce inappropriate usage of stress ulcer prophylaxis in hospitalized patients
Abstract
Aims: To promote effective methods to improve overutilization patterns of acid-suppressive therapy in hospitalized patients and to evaluate the impact of multidisciplinary team efforts to reduce inappropriate use of stress ulcer prophylaxis in low-risk patients.
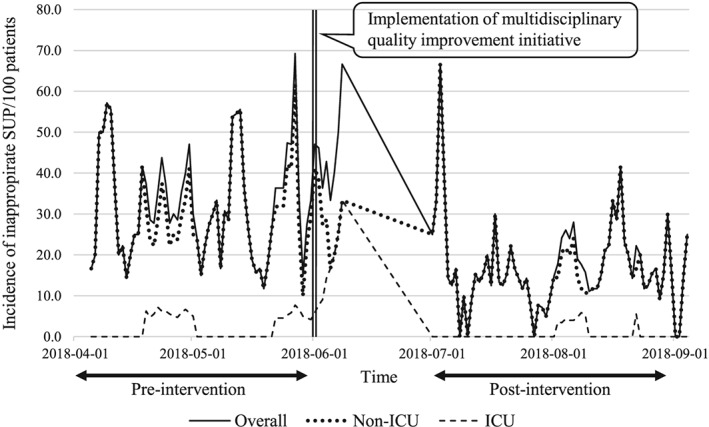
Methods: A multidisciplinary quality improvement initiative incorporating education, medication use reviews and reconciliation, and pharmaceutical intervention was implemented in June 2018 for surgical patients hospitalized via emergency department. For the pre-post analysis and time series analysis, patients admitted during April and May were classified into the pre-intervention cohort and those admitted during July and August into the post-intervention cohort.
Results: Three hundred and seventeen patients were included in this study (153 and 164 in the pre- and post-intervention cohorts, respectively). The multidisciplinary program was effective in reducing overuse of stress ulcer prophylaxis and healthcare expenses associated with it. Biweekly education on risk factors warranting stress ulcer prophylaxis was provided for clinicians, and acid-suppressive therapy was removed from a preset list of admission orders. The incidence of inappropriate prophylaxis use declined substantially following intervention in overall patients (OR = 0.51, P = 0.01) and a significant decrease was primarily observed among non-ICU patients (OR = 0.50, P = 0.01). Interrupted time series analysis confirmed the significant decline in inappropriate use post intervention (coefficient = -0.63, P < 0.001). The total healthcare expenses associated with such overuse decreased by 58.5% from US$ 19.39 to US$ 8.04 per 100 patient-days.
Conclusions: Our multidisciplinary team efforts were associated with improvement in stress ulcer prophylaxis overuse patterns, resulting in a substantial decrease in the incidence of inappropriate use, especially in general wards, and associated healthcare costs.
Keywords: acid suppression; multidisciplinary; quality improvement; stress ulcer prophylaxis.
© 2019 The British Pharmacological Society.
Conflict of interest statement
There are no competing interests to declare.
Figures
Similar articles
-
An interprofessional approach to reducing the overutilization of stress ulcer prophylaxis in adult medical and surgical intensive care units.Ann Pharmacother. 2014 Apr;48(4):462-9. doi: 10.1177/1060028013517088. Epub 2014 Jan 28. Ann Pharmacother. 2014. PMID: 24473490
-
Impact of a clinical pharmacist stress ulcer prophylaxis management program on inappropriate use in hospitalized patients.Am J Med. 2015 Aug;128(8):905-13. doi: 10.1016/j.amjmed.2015.02.014. Epub 2015 Mar 27. Am J Med. 2015. PMID: 25820164
-
Effects of pharmacy resident led education on resident physician prescribing habits associated with stress ulcer prophylaxis in non-intensive care unit patients.Am J Health Syst Pharm. 2015 Jun 1;72(11 Suppl 1):S48-52. doi: 10.2146/sp150013. Am J Health Syst Pharm. 2015. PMID: 25991596
-
Stress ulcer prophylaxis in hospitalized patients not in intensive care units.Am J Health Syst Pharm. 2007 Jul 1;64(13):1396-400. doi: 10.2146/ajhp060393. Am J Health Syst Pharm. 2007. PMID: 17592004 Review.
-
Stress-ulcer prophylaxis for general medical patients: a review of the evidence.J Hosp Med. 2007 Mar;2(2):86-92. doi: 10.1002/jhm.177. J Hosp Med. 2007. PMID: 17427249 Review.
Cited by
-
Appropriateness and inappropriate medication predictors of stress ulcer prophylaxis in the intensive care unit.Front Pharmacol. 2025 Jan 7;15:1401335. doi: 10.3389/fphar.2024.1401335. eCollection 2024. Front Pharmacol. 2025. PMID: 39840110 Free PMC article.
-
Impact of institutional quality improvement initiatives on metabolic monitoring in mental disorder in patients treated with antipsychotics: A meta-analysis of intervention studies.J Glob Health. 2024 May 24;14:04074. doi: 10.7189/jogh.14.04074. J Glob Health. 2024. PMID: 38783701 Free PMC article.
-
Prevalence and factors associated with inappropriate continuation of stress ulcer prophylaxis at discharge.BMJ Open Qual. 2024 May 10;13(2):e002678. doi: 10.1136/bmjoq-2023-002678. BMJ Open Qual. 2024. PMID: 38729753 Free PMC article.
References
-
- Mutlu GM, Mutlu EA, Factor P. GI complications in patients receiving mechanical ventilation. Chest. 2001;119(4):1222‐1241. - PubMed
-
- Cook DJ, Fuller HD, Guyatt GH, et al. Lacroix, J, Griffith L, Willan a; Canadian critical care trials group. Risk factors for gastrointestinal bleeding in critically ill patients. Canadian critical trials group. N Engl J Med. 1994;330(6):377‐381. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
