

Acyclovir for Mechanically Ventilated Patients With Herpes Simplex Virus Oropharyngeal Reactivation: A Randomized Clinical Trial
- PMID: 31841577
- PMCID: PMC6990840
- DOI: 10.1001/jamainternmed.2019.5713
Acyclovir for Mechanically Ventilated Patients With Herpes Simplex Virus Oropharyngeal Reactivation: A Randomized Clinical Trial
Abstract
Importance: The role of herpes simplex virus (HSV) reactivation on morbidity and mortality in patients in the intensive care unit requiring mechanical ventilation remains unknown.
Objective: To determine whether preemptive treatment with intravenous acyclovir reduces the duration of mechanical ventilation in patients with HSV oropharyngeal reactivation.
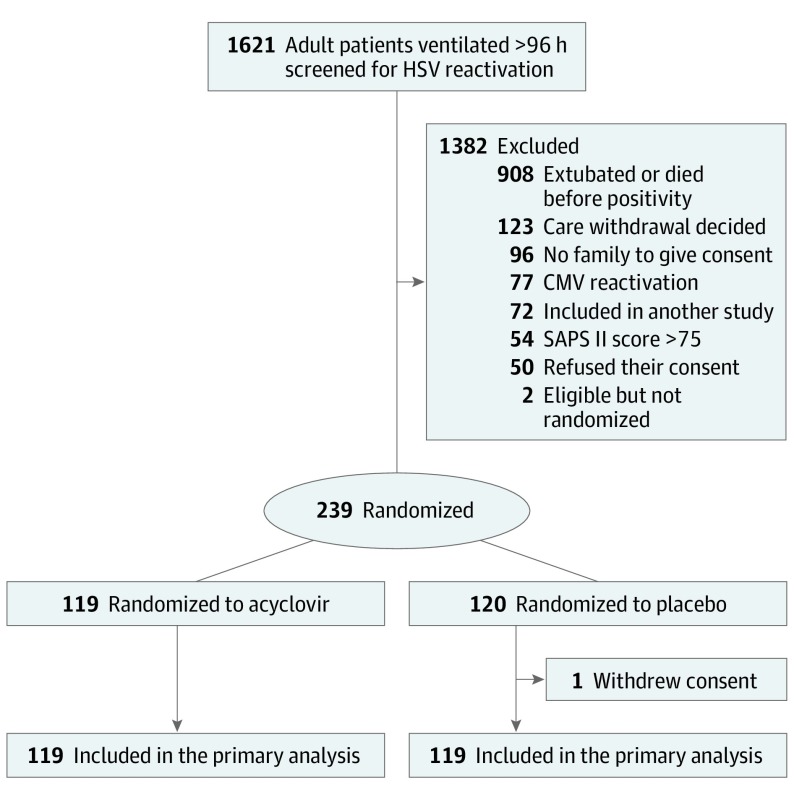
Design, setting, and participants: A double-blind, placebo-controlled randomized clinical trial was conducted in 16 intensive care units in France. Participants included 239 adults (age, >18 years) who received mechanical ventilation for at least 96 hours and continued to receive mechanical ventilation for 48 hours or more, with HSV oropharyngeal reactivation. Patients were enrolled between February 2, 2014, and February 22, 2018.
Interventions: Participants were randomized to receive intravenous acyclovir, 5 mg/kg, 3 times daily for 14 days or a matching placebo.
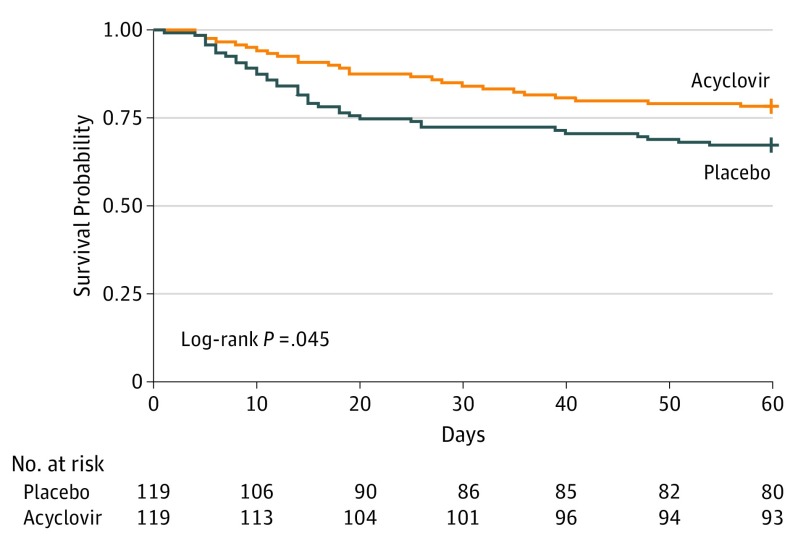
Main outcomes and measures: The primary end point was ventilator-free days from randomization to day 60. Prespecified secondary outcomes included mortality at 60 days. Main analyses were conducted on an intention-to-treat basis.
Results: Of 239 patients enrolled and randomized, 1 patient withdrew consent, leaving 238 patients, with 119 patients in both the acyclovir and placebo (control) groups (median [IQR] age, 61 [50-70] years; 76 [32%] women) available for primary outcome measurement. On day 60, the median (IQR) numbers of ventilator-free days were 35 (0-53) for acyclovir recipients and 36 (0-50]) for controls (P = .17 for between-group comparison). Among secondary outcomes, 26 patients (22%) and 39 patients (33%) had died at day 60 (risk difference, 0.11, 95% CI, -0.004 to 0.22, P = .06). The adverse event frequency was similar for both groups (28% in the acyclovir group and 23% in the placebo group, P = .40), particularly acute renal failure post randomization affecting 3 acyclovir recipients (3%) and 2 controls (2%). Four patients (3%) in the acyclovir group vs none in the placebo group stopped the study drug for treatment-related adverse events.
Conclusions and relevance: In patients receiving mechanical ventilation for 96 hours or more with HSV reactivation in the throat, use of acyclovir, 5 mg/kg, 3 times daily for 14 days, did not increase the number of ventilator-free days at day 60, compared with placebo. These findings do not appear to support routine preemptive use of acyclovir in this setting.
Trial registration: ClinicalTrials.gov identifier: NCT02152358.
Conflict of interest statement
Figures
Comment in
-
Preemptive Treatment of Herpes Simplex Virus Reactivation in Critically Ill Patients?-Not Based on Current Data.JAMA Intern Med. 2020 Feb 1;180(2):272-273. doi: 10.1001/jamainternmed.2019.6423. JAMA Intern Med. 2020. PMID: 31841575 No abstract available.
