

Association between the location of transposed ovary and ovarian dose in patients with cervical cancer treated with postoperative pelvic radiotherapy
- PMID: 31842971
- PMCID: PMC6916465
- DOI: 10.1186/s13014-019-1437-3
Association between the location of transposed ovary and ovarian dose in patients with cervical cancer treated with postoperative pelvic radiotherapy
Abstract
Background and purpose: How to protect the ovarian function during radiotherapy is uncertain. The purpose of this study was to explore the association between the location of the transposed ovary and the ovarian dose in patients with cervical cancer received radical hysterectomy, ovarian transposition, and postoperative pelvic radiotherapy.
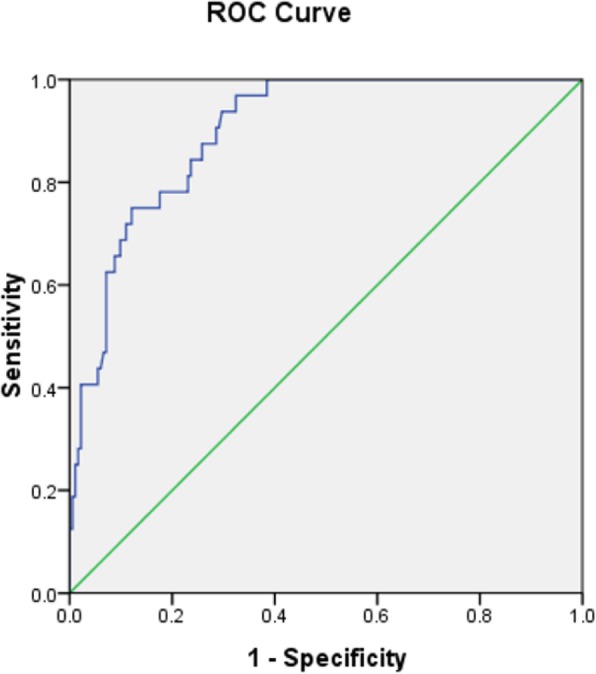
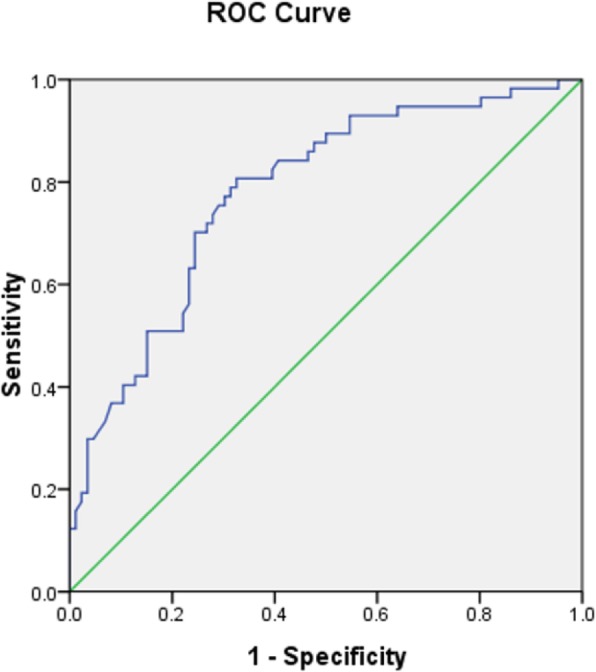
Methods: A retrospective analysis was conducted of 150 young patients with cervical cancer who received radical hysterectomy, intraoperative ovarian transposition, and postoperative adjuvant radiotherapy in Zhejiang Cancer Hospital. Association between location of the transposed ovaries and ovarian dose was evaluated. The transposed position of ovaries with a satisfactory dose was explored using a receiver operator characteristic curve (ROC) analysis. Patients' ovarian function was followed up 3 months and 1 year after radiotherapy.
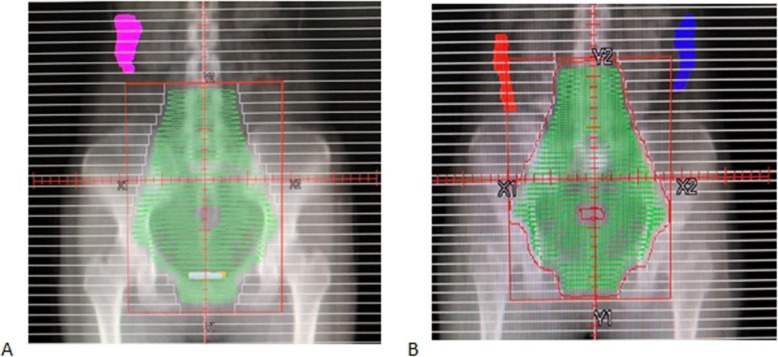
Results: A total of 32/214 (15%) transposed ovaries were higher than the upper boundary of the planning target volume (PTV). The optimum cutoff value of > 1.12 cm above the iliac crest plane was significantly associated with ovaries above the upper PTV boundary. When the ovaries were below the upper boundary of PTV, the optimum cutoff value of transverse distance > 3.265 cm between the ovary and PTV was significantly associated with ovarian max dose (Dmax) ≤ 4Gy, and the optimum cutoff value of transverse distance > 2.391 cm was significantly associated with ovarian Dmax≤5Gy. A total of 77 patients had received complete follow-up, and 56 patients (72.7%) showed preserved ovarian function 1 year after radiotherapy, which was significantly increased compared with 3 months (44.2%) after radiotherapy.
Conclusions: The location of transposed ovaries in patients with cervical cancer is significantly correlated with ovarian dose in adjuvant radiotherapy. We recommend transposition of ovaries > 1.12 cm higher than the iliac crest plane to obtain ovarian location above PTV. When the transposed ovary is below the upper boundary of PTV, ovarian Dmax ≤4Gy may be obtained when the transverse distance between the ovary and PTV was > 3.265 cm, and the ovarian Dmax≤5Gy may be obtained when the transverse distance was > 2.391 cm.
Keywords: Dose limit; Ovarian function; Ovarian transposition; Pelvic radiotherapy; Uterine cervical neoplasms.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. - PubMed
