

Detection of PLA2R Autoantibodies before the Diagnosis of Membranous Nephropathy
- PMID: 31843984
- PMCID: PMC6934991
- DOI: 10.1681/ASN.2019050538
Detection of PLA2R Autoantibodies before the Diagnosis of Membranous Nephropathy
Abstract
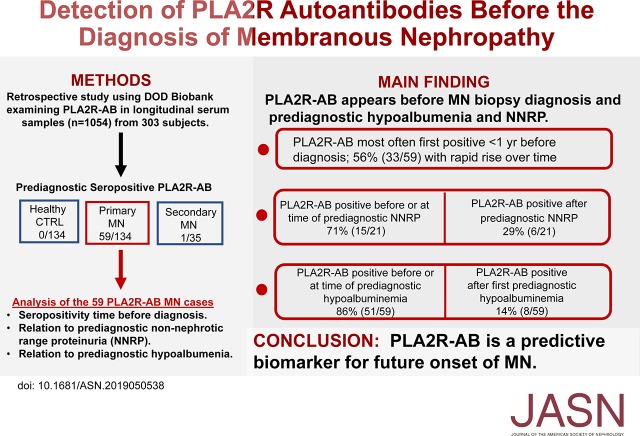
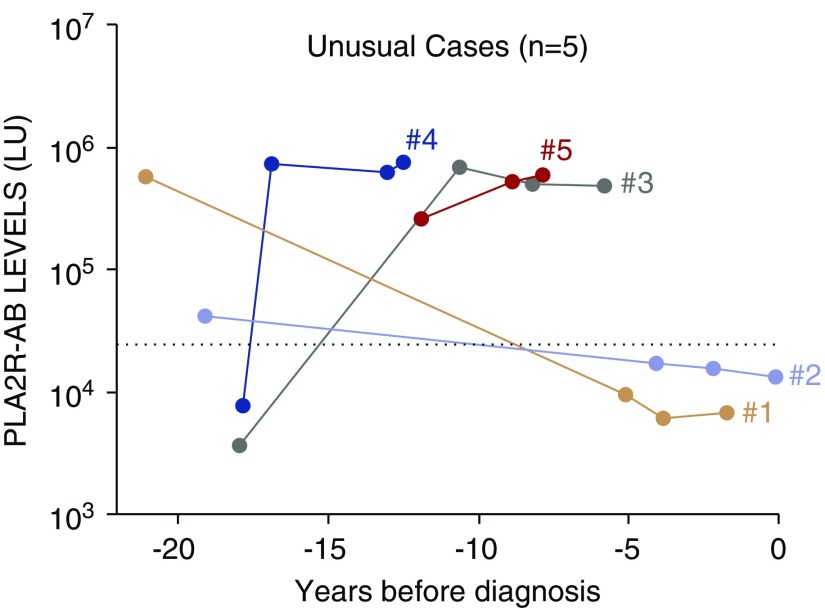
Background: Circulating serum autoantibodies against the M-type phospholipase A2 receptor (PLA2R-AB) are a key biomarker in the diagnosis and monitoring of primary membranous nephropathy (MN). However, little is known about the appearance and trajectory of PLA2R-AB before the clinical diagnosis of MN.
Methods: Using the Department of Defense Serum Repository, we analyzed PLA2R-AB in multiple, 1054 longitudinal serum samples collected before diagnosis of MN from 134 individuals with primary MN, 35 individuals with secondary MN, and 134 healthy volunteers. We evaluated the presence and timing of non-nephrotic range proteinuria (NNRP) and serum albumin measurements in relation to PLA2R-AB status.
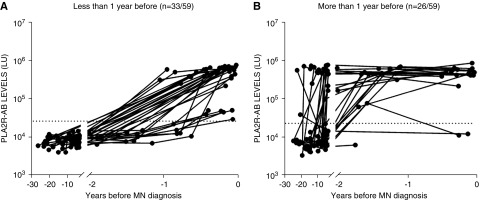
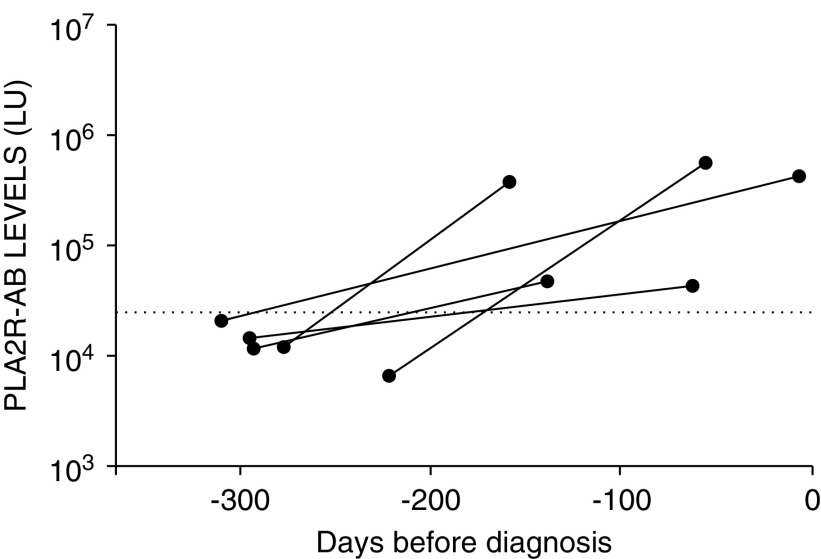
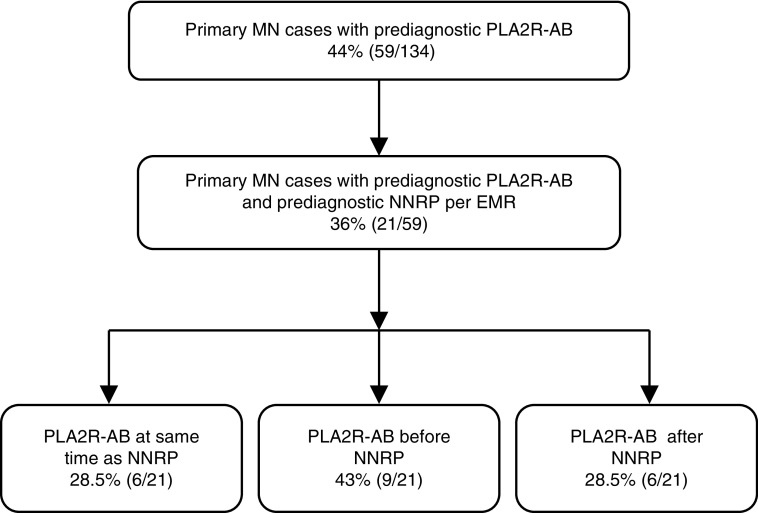
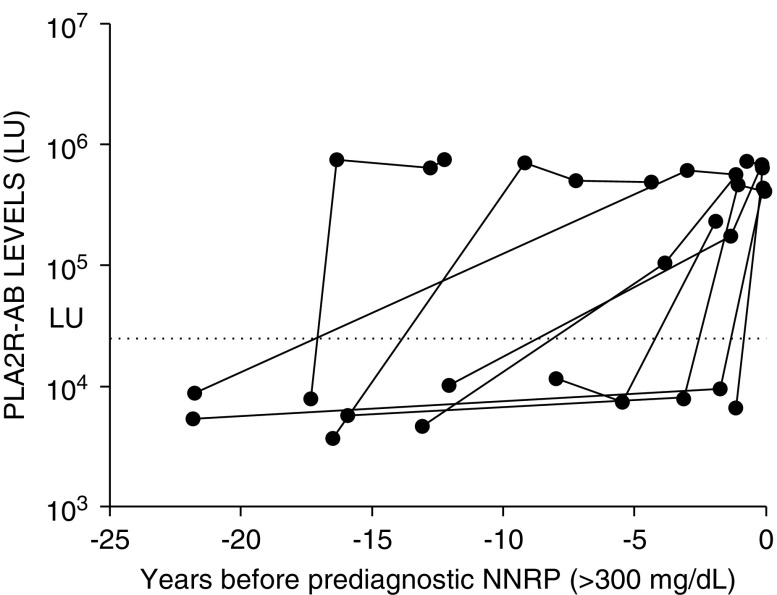
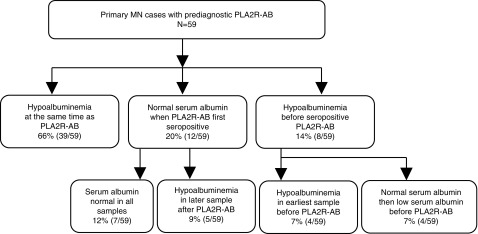
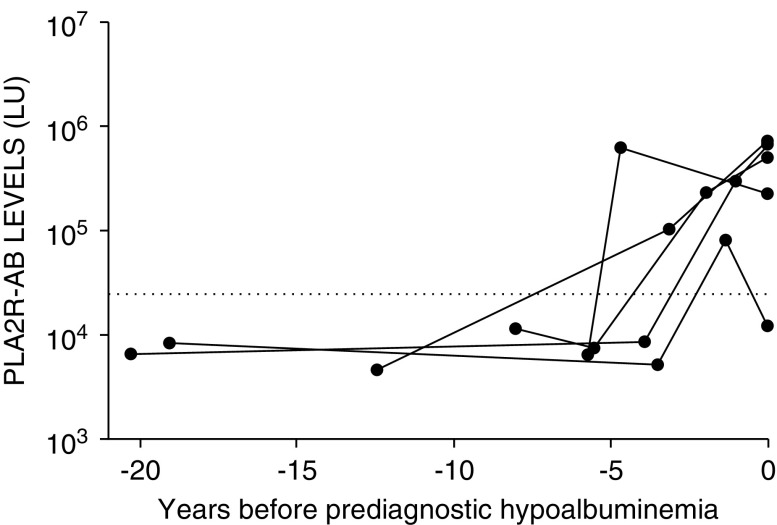
Results: Analysis of PLA2R-AB in longitudinal serum samples revealed seropositivity in 44% (59 out of 134) of primary MN cases, 3% (one out of 35) of secondary MN cases, and in 0% of healthy controls. Among patients with MN, PLA2R-AB were detectable at a median of 274 days before renal biopsy diagnosis (interquartile range, 71-821 days). Approximately one third of the participants became seropositive within 3 months of MN diagnosis. Of the 21 individuals with documented prediagnostic NNRP, 43% (nine out of 21) were seropositive before NNRP was first documented and 28.5% (six out of 21) were seropositive at the same time as NNRP; 66% (39 out of 59) of those seropositive for PLA2R-AB had hypoalbuminemia present at the time antibody was initially detected. Twelve participants (20%) were seropositive before hypoalbuminemia became apparent, and eight participants (14%) were seropositive after hypoalbuminemia became apparent.
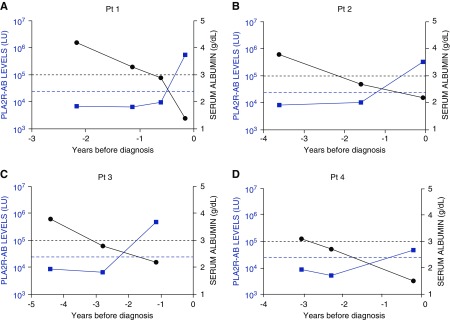
Conclusions: Circulating PLA2R-AB are detectable months to years before documented NNRP and biopsy-proven diagnosis in patients with MN.
Keywords: glomerular disease; glomerulopathy; membranous nephropathy; nephrotic syndrome; proteinuria.
Copyright © 2020 by the American Society of Nephrology.
Figures
Comment in
-
Refining Our Understanding of the PLA2R-Antibody Response in Primary Membranous Nephropathy: Looking Forward, Looking Back.J Am Soc Nephrol. 2020 Jan;31(1):8-11. doi: 10.1681/ASN.2019111195. Epub 2019 Dec 16. J Am Soc Nephrol. 2020. PMID: 31871252 Free PMC article. No abstract available.
References
-
- Ronco P, Debiec H: Pathophysiological advances in membranous nephropathy: Time for a shift in patient’s care. Lancet 385: 1983–1992, 2015 - PubMed
-
- Ancian P, Lambeau G, Mattéi MG, Lazdunski M: The human 180-kDa receptor for secretory phospholipases A2. Molecular cloning, identification of a secreted soluble form, expression, and chromosomal localization. J Biol Chem 270: 8963–8970, 1995 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
