

The upper-airway microbiota and loss of asthma control among asthmatic children
- PMID: 31844063
- PMCID: PMC6915697
- DOI: 10.1038/s41467-019-13698-x
The upper-airway microbiota and loss of asthma control among asthmatic children
Abstract
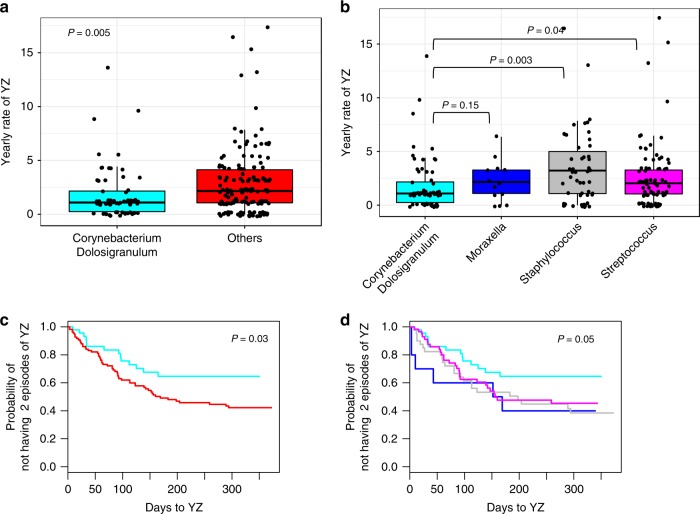
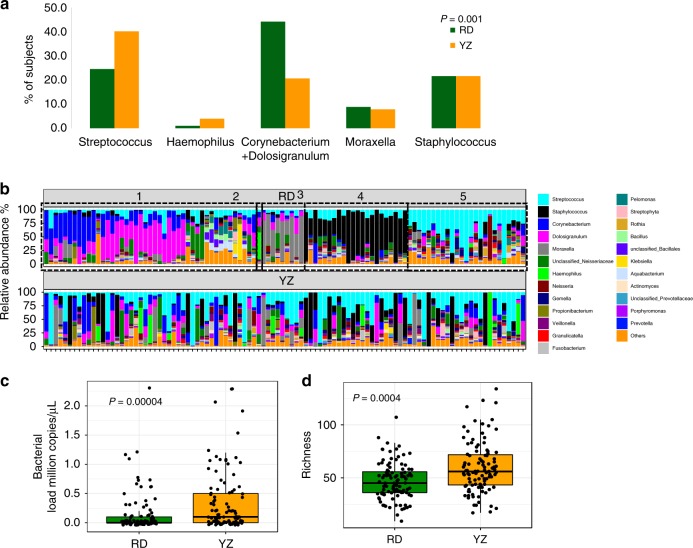
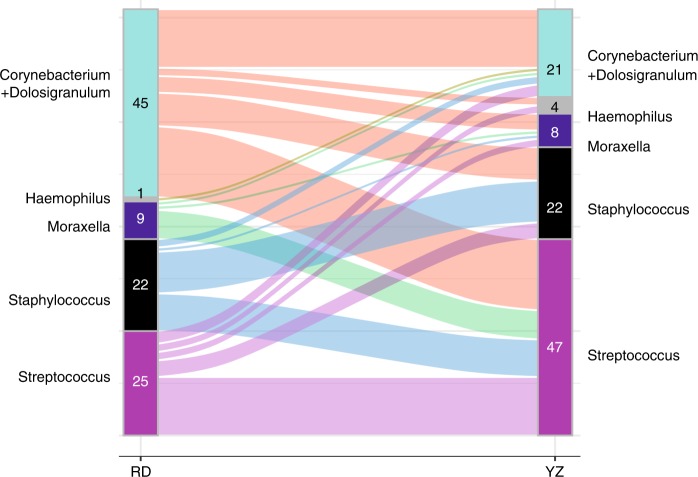
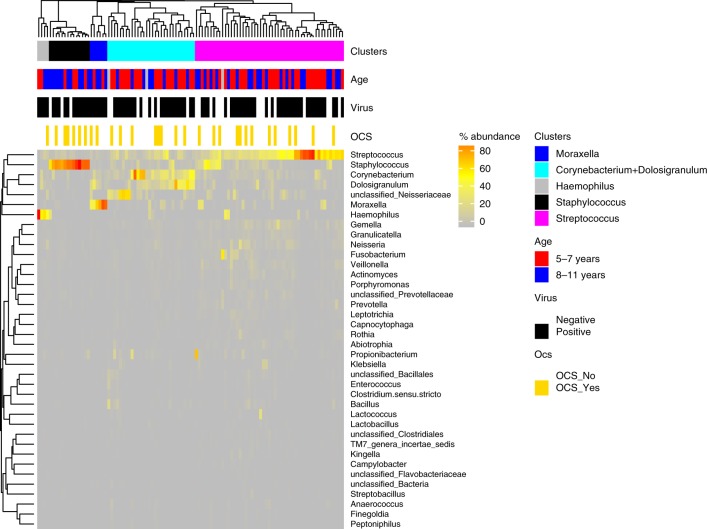
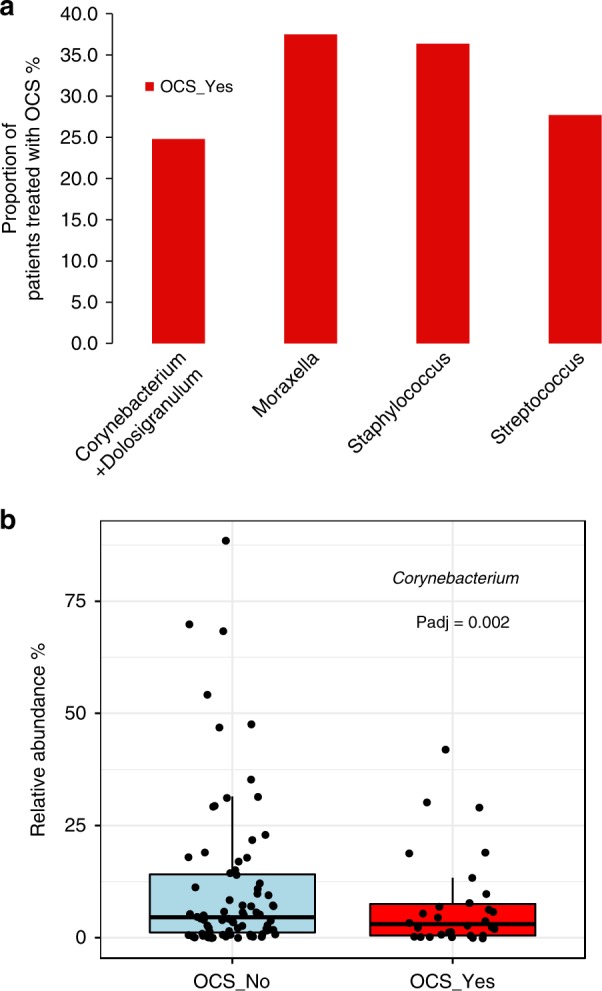
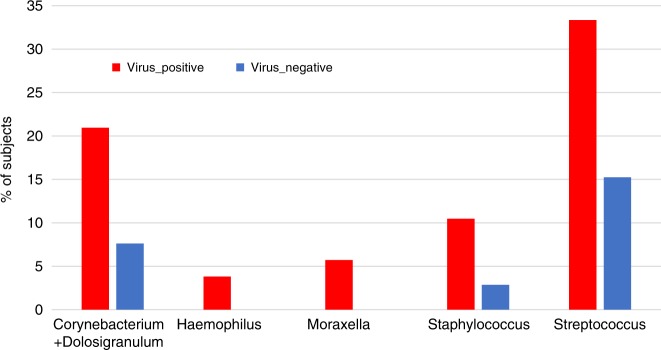
The airway microbiome has an important role in asthma pathophysiology. However, little is known on the relationships between the airway microbiome of asthmatic children, loss of asthma control, and severe exacerbations. Here we report that the microbiota's dynamic patterns and compositions are related to asthma exacerbations. We collected nasal blow samples (n = 319) longitudinally during a clinical trial at 2 time-points within one year: randomization when asthma is under control, and at time of early loss of asthma control (yellow zone (YZ)). We report that participants whose microbiota was dominated by the commensal Corynebacterium + Dolosigranulum cluster at RD experience the lowest rates of YZs (p = 0.005) and have longer time to develop at least 2 episodes of YZ (p = 0.03). The airway microbiota have changed from randomization to YZ. A switch from the Corynebacterium + Dolosigranulum cluster at randomization to the Moraxella- cluster at YZ poses the highest risk of severe asthma exacerbation (p = 0.04). Corynebacterium's relative abundance at YZ is inversely associated with severe exacerbation (p = 0.002).
Conflict of interest statement
D.J.: declares receiving research grants from NHLBI, NIAID, and GlaxoSmithKline. He has received personal fees for a DSMB from Pfizer, and for advisory boards from Novartis, GlaxoSmithKline, AstraZenena, Sanofi-Regeneron, Boehringer Ingelheim, and Vifor pharma. L.B.B.: declares receiving research grants from NIH, NHLBI, NIAID. He has received personal fees from GlaxoSmithKline, Genentech, Novartis, Merck, DBV technologies, Teva, Boehringer Ingelheim, Sanofi, Regeneron, AstraZenena, Vectura, Circassia. M.C.: pharmaceutical grant funding from AstraZenena, Chiesi, Novartis, GSK, Sanofi. Consultant for Genentech, Theravance, VIAA, Teva, Sanofi, Novartis. Speaker for AstraZenena, Genentech, GSK, Regeneron, Sanofi, Teva. Received royalties from Elsevier. Y.H.: research support from the NIH for microbiome research. R.F.L.: research support from the NIH for microbiome research. W.P.: Consultant for Novartis, Genentech, Regeneron, GSK, Teva, Sanofi. R.G.R.: research support from the NIH. The remaining authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
