

Usefulness of a multibending endoscope in gastric endoscopic submucosal dissection
- PMID: 31844823
- PMCID: PMC6895728
- DOI: 10.1016/j.vgie.2019.08.012
Usefulness of a multibending endoscope in gastric endoscopic submucosal dissection
Abstract
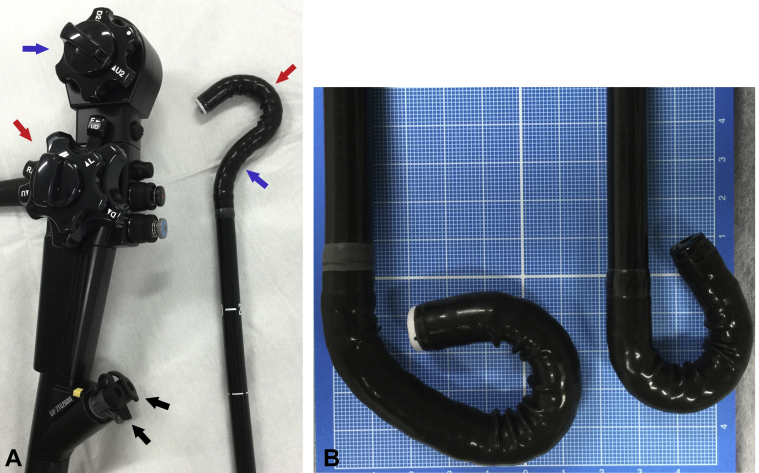
Background and aims: Intraoperative perforation is a major adverse event of endoscopic submucosal dissection (ESD). To avoid perforation, it is important for the endoscope to approach the portion to be resected carefully and to ensure that the knife can approach the submucosa at an angle parallel to the muscle layer. The multibending endoscope has 2 bends at its tip and may facilitate the ESD procedure. To the best of our knowledge, very few studies have reported the use of the multibending endoscope during gastric ESD. The aim of this study was, therefore, to introduce the usefulness of the multibending endoscope for gastric ESD.
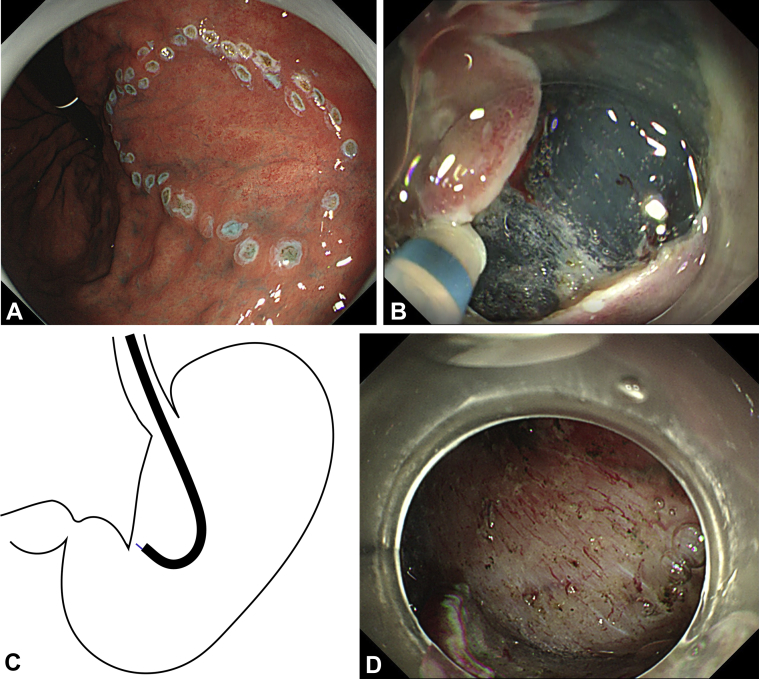
Methods: We report 2 cases of early gastric cancer in which ESD was performed using a multibending endoscope.
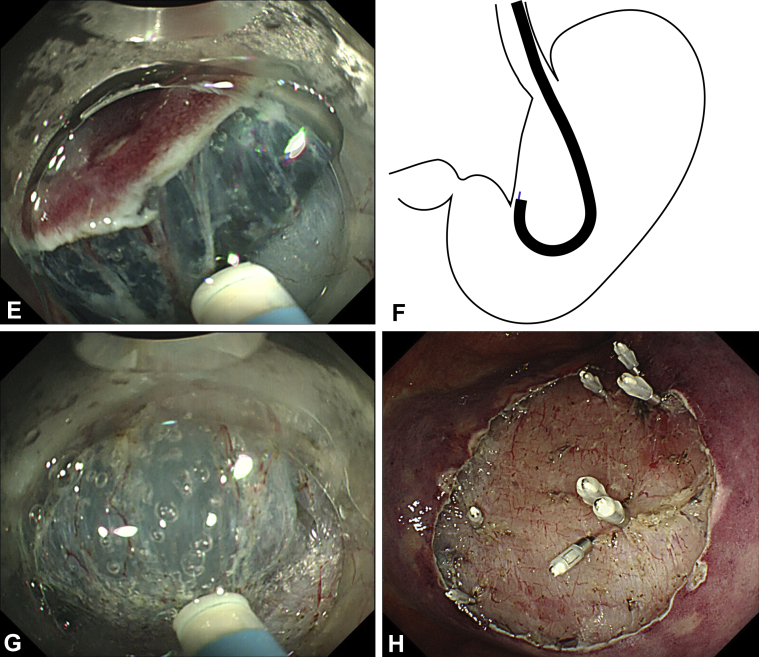
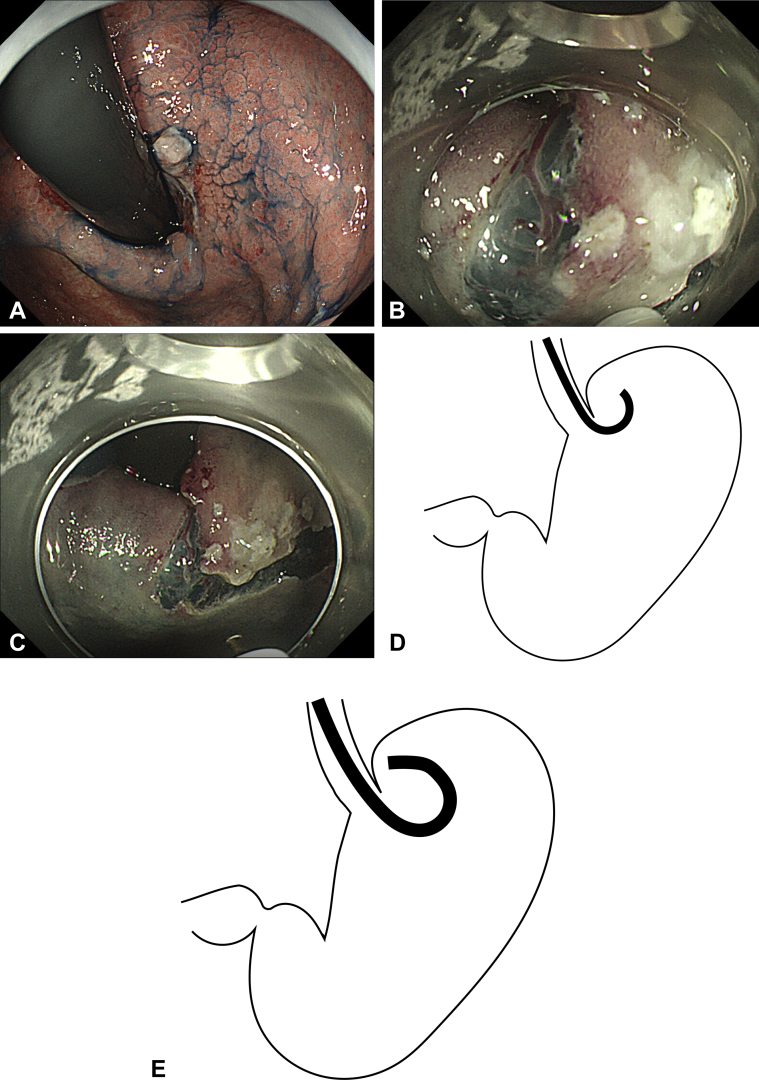
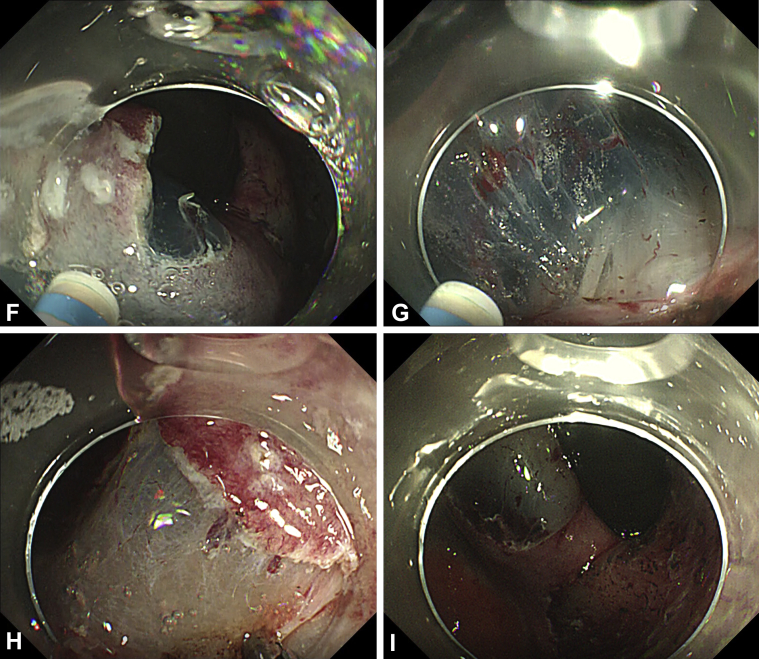
Results: Unlike conventional single-bending endoscopes that have only 1 moveable part, the multibending endoscope allowed difficult areas to be approached more easily. Small adjustments could be made to the upward or downward angle of both the first and the second bending sections of the endoscope. This ensured that the knife would approach the submucosa at an angle parallel to the muscle layer. In patient 1, initially the conventional endoscope was used, but it became more difficult to approach the site, and paradoxic movement occurred. When the conventional endoscope was changed to the multibending endoscope, the ESD procedure became safer and more efficient. Another ESD using the multibending endoscope was performed successfully without any adverse events.
Conclusions: The use of a multibending endoscope for ESD will enable safer and faster treatment of patients.
Keywords: ESD, endoscopic submucosal dissection.
© 2019 American Society for Gastrointestinal Endoscopy. Published by Elsevier Inc.
Figures
References
-
- Yamamoto Y., Kikuchi D., Nagami Y. Management of adverse events related to endoscopic resection of upper gastrointestinal neoplasms: review of the literature and recommendations from experts. Dig Endosc. 2019;31:4–20. - PubMed
-
- Daegu-Kyungpook Gastrointestinal Study Group (DGSG) Kim M., Jeon S.W., Cho K.B. Predictive risk factors of perforation in gastric endoscopic submucosal dissection for early gastric cancer: a large, multicenter study. Surg Endosc. 2013;27:1372–1378. - PubMed
-
- Imagawa A., Okada H., Kawahara Y. Endoscopic submucosal dissection for early gastric cancer: results and degrees of technical difficulty as well as success. Endoscopy. 2006;38:987–990. - PubMed
-
- Kawamura M., Sekine H., Kikuchi T. Endoscopic submucosal dissection for gastric neoplasms by using a novel attachment device-a one-sided, expandable balloon. Gastrointest Endosc. 2011;74:415–418. - PubMed
-
- Isshi K., Tajiri H., Fujisaki J. The effectiveness of a new multibending scope for endoscopic mucosal resection. Endoscopy. 2004;36:294–297. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
