

Incorporation of molecular characteristics into endometrial cancer management
- PMID: 31846532
- PMCID: PMC6972558
- DOI: 10.1111/his.14015
Incorporation of molecular characteristics into endometrial cancer management
Abstract
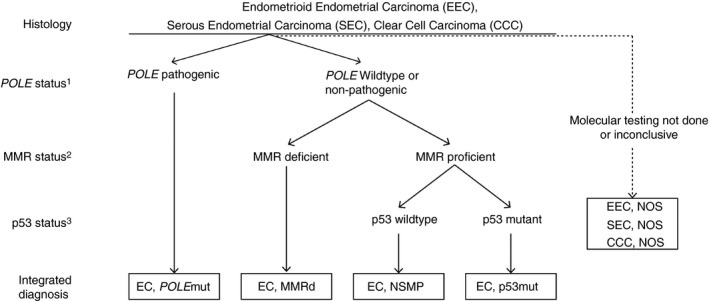
Histopathological evaluation including subtyping and grading is the current cornerstone for endometrial cancer (EC) classification. This provides clinicians with prognostic information and input for further treatment recommendations. Nonetheless, patients with histologically similar ECs may have very different outcomes, notably in patients with high-grade endometrial carcinomas. For endometrial cancer, four molecular subgroups have undergone extensive studies in recent years: POLE ultramutated (POLEmut), mismatch repair-deficient (MMRd), p53 mutant (p53abn) and those EC lacking any of these alterations, referred to as NSMP (non-specific molecular profile). Several large studies confirm the prognostic relevance of these molecular subgroups. However, this 'histomolecular' approach has so far not been implemented in clinical routine. The ongoing PORTEC4a trial is the first clinical setting in which the added value of integrating molecular parameters in adjuvant treatment decisions will be determined. For diagnostics, the incorporation of the molecular parameters in EC classification will add a level of objectivity which will yield biologically more homogeneous subclasses. Here we illustrate how the management of individual EC patients may be impacted when applying the molecular EC classification. We describe our current approach to the integrated diagnoses of EC with a focus on scenarios with conflicting morphological and molecular findings. We also address several pitfalls accompanying the diagnostic implementation of molecular EC classification and give practical suggestions for diagnostic scenarios.
Keywords: POLE; adjuvant treatment; endometrial carcinoma; lymphovascular space invasion; mismatch repair; molecular classification; p53; risk stratification.
© 2019 The Authors. Histopathology published by John Wiley & Sons Ltd.
Conflict of interest statement
All authors declare no conflicts of interest.
Figures

References
-
- Kurman RJ, Carcangiu ML, Herrington S, Young RH. WHO classification of tumours of female reproductive organs. 4th ed Lyon: WHO Press, 2014.
-
- Gilks CB, Oliva E, Soslow RA. Poor interobserver reproducibility in the diagnosis of high‐grade endometrial carcinoma. Am. J. Surg. Pathol. 2013; 37; 874–881. - PubMed
-
- Stelloo E, Nout RA, Osse EM et al Improved risk assessment by integrating molecular and clinicopathological factors in early‐stage endometrial cancer‐combined analysis of the portec cohorts. Clin. Cancer Res. 2016; 22; 4215–4224. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
