

Coverage of immediate postpartum long-acting reversible contraception has improved birth intervals for at-risk populations
- PMID: 31846612
- PMCID: PMC7147501
- DOI: 10.1016/j.ajog.2019.11.1282
Coverage of immediate postpartum long-acting reversible contraception has improved birth intervals for at-risk populations
Abstract
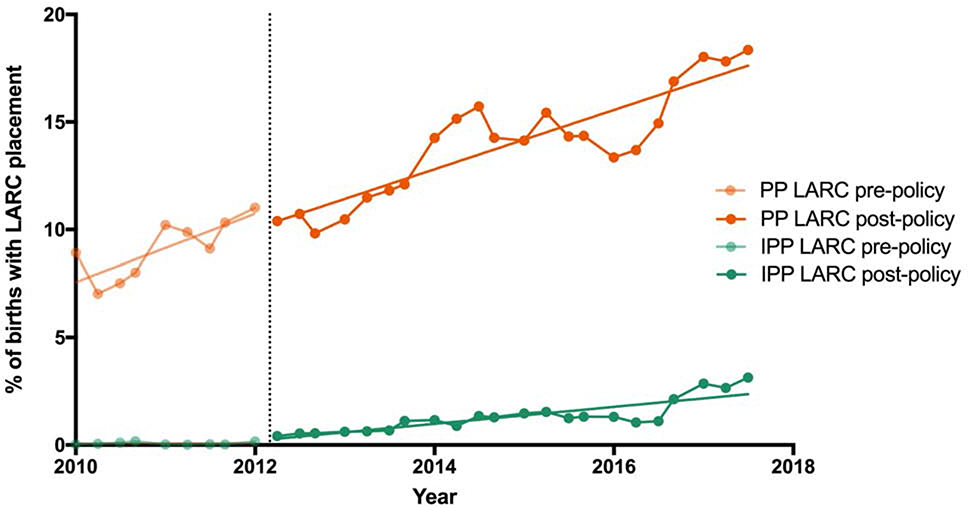
Background: In 2012, South Carolina revised the Medicaid policy to cover reimbursement for immediate postpartum long-acting reversible contraception. Immediate postpartum long-acting reversible contraception may improve health outcomes for populations at risk with a subsequent short-interval pregnancy.
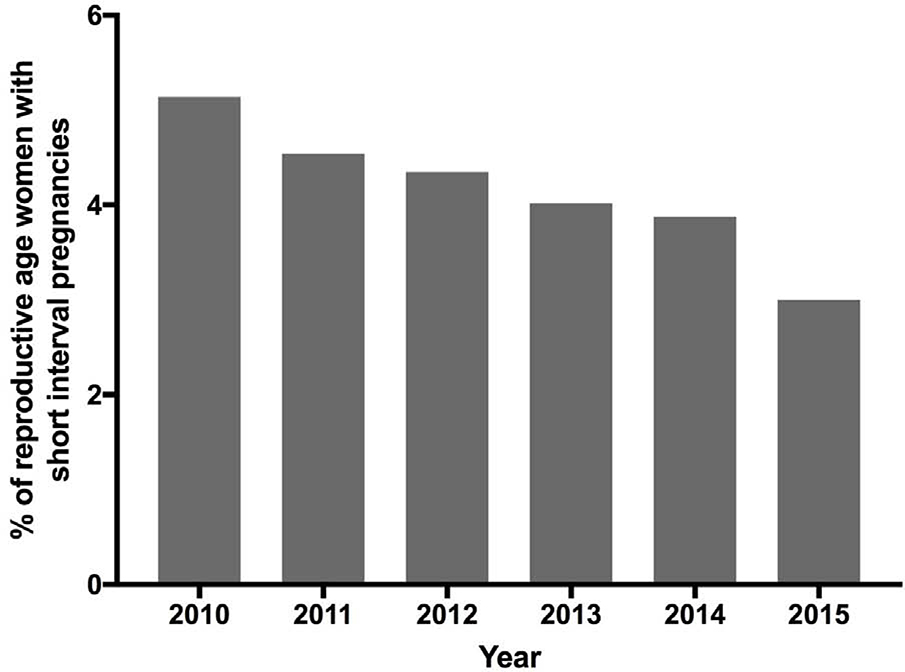
Objectives: We examined the impact of the Medicaid policy change on the initiation of long-acting and reversible contraception (immediate postpartum and postpartum) within key populations. We determined whether immediate postpartum long-acting and reversible contraception use varied by adequate prenatal care (>7 visits), metropolitan location, and medical comorbidities. We also tested the association of immediate postpartum and postpartum long-acting, reversible contraception on interpregnancy interval of less than 18 months.
Study design: We conducted a historical cohort study of live births among Medicaid recipients in South Carolina between 2010 and 2017, 2 years before and 5 years after the policy change. We used birth certificate data linked with Medicaid claims. Our primary outcome was immediate postpartum long-acting and reversible contraception, and our secondary outcome was short interpregnancy interval. We characterize trends in long-acting and reversible contraception use and interpregnancy interval over the study period. We used logistic regression models to test the association of key factors (rural, inadequate prenatal care, and medical comorbidities) with immediate and outpatient postpartum long-acting and reversible contraception following the policy change and to test the association of immediate postpartum and postpartum long-acting and reversible contraception with short interpregnancy interval.
Results: Our sample included 187,438 births to 145,973 women. Overall, 44.7% of the sample was white, with a mean age of 25.0 years. A majority of the sample (61.5%) was multiparous and resided in metropolitan areas (79.5%). The odds of receipt of immediate postpartum long-acting and reversible contraception use increased after the policy change (adjusted odds ratio, 1.39, 95% confidence interval, 1.34-1.43). Women with inadequate prenatal care (adjusted odds ratio, 1.50, 95% confidence interval, 1.31-1.71) and medically complex pregnancies had higher odds of receipt of immediate postpartum long-acting and reversible contraception following the policy change (adjusted odds ratio, 1.47, 95% confidence interval, 1.29-1.67) compared with women with adequate prenatal care and normal pregnancies. Women residing in rural areas were less likely to receive immediate postpartum long-acting and reversible contraception (adjusted odds ratio, 0.36, 95% confidence interval, 0.30-0.44) than women in metropolitan areas. Utilization of immediate postpartum long-acting and reversible contraception was associated with a decreased odds of a subsequent short interpregnancy interval (adjusted odds ratio, 0.62, 95% confidence interval, 0.44-0.89).
Conclusion: Women at risk of a subsequent pregnancy and complications (inadequate prenatal care and medical comorbidities) are more likely to receive immediate postpartum long-acting and reversible contraception following the policy change. Efforts are needed to improve access in rural areas.
Keywords: Medicaid policy; immediate postpartum long-acting reversible contraception; implant; intrauterine device; short interpregnancy intervals.
Copyright © 2019 Elsevier Inc. All rights reserved.
Figures
References
-
- Hanley GE, Hutcheon JA, Kinniburgh BA, Lee L. Interpregnancy Interval and Adverse Pregnancy Outcomes: An Analysis of Successive Pregnancies. Obstet Gynecol 2017;129:408–15. - PubMed
-
- Conde-Agudelo A, Rosas-Bermúdez A, Kafury-Goeta A. Birth Spacing and Risk of Adverse Perinatal Outcomes A Meta-analysis. JAMA 2006;295:1809–23. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
