

Financing intersectoral action for health: a systematic review of co-financing models
- PMID: 31849335
- PMCID: PMC6918645
- DOI: 10.1186/s12992-019-0513-7
Financing intersectoral action for health: a systematic review of co-financing models
Abstract
Background: Addressing the social and other non-biological determinants of health largely depends on policies and programmes implemented outside the health sector. While there is growing evidence on the effectiveness of interventions that tackle these upstream determinants, the health sector does not typically prioritise them. From a health perspective, they may not be cost-effective because their non-health outcomes tend to be ignored. Non-health sectors may, in turn, undervalue interventions with important co-benefits for population health, given their focus on their own sectoral objectives. The societal value of win-win interventions with impacts on multiple development goals may, therefore, be under-valued and under-resourced, as a result of siloed resource allocation mechanisms. Pooling budgets across sectors could ensure the total multi-sectoral value of these interventions is captured, and sectors' shared goals are achieved more efficiently. Under such a co-financing approach, the cost of interventions with multi-sectoral outcomes would be shared by benefiting sectors, stimulating mutually beneficial cross-sectoral investments. Leveraging funding in other sectors could off-set flat-lining global development assistance for health and optimise public spending. Although there have been experiments with such cross-sectoral co-financing in several settings, there has been limited analysis to examine these models, their performance and their institutional feasibility.
Aim: This study aimed to identify and characterise cross-sectoral co-financing models, their operational modalities, effectiveness, and institutional enablers and barriers.
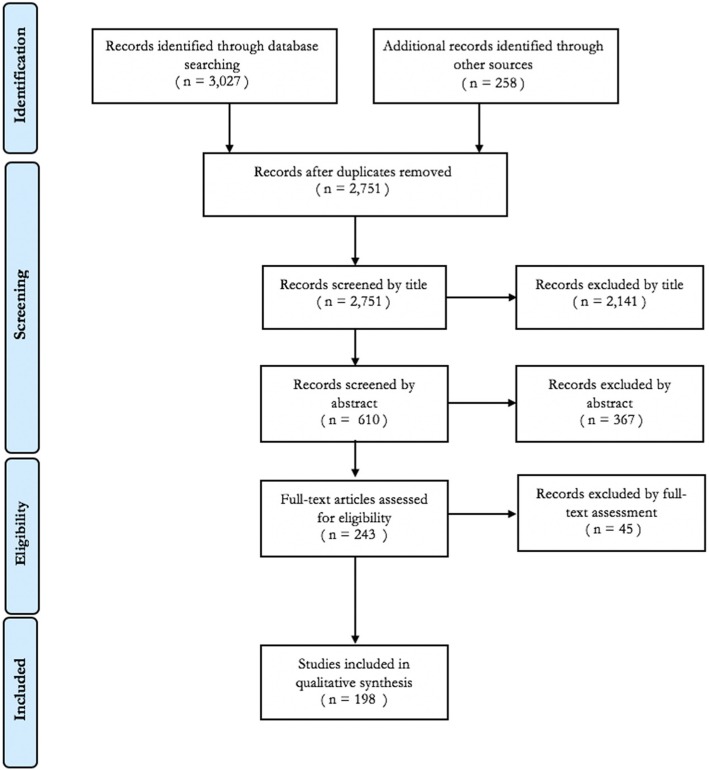
Methods: We conducted a systematic review of peer-reviewed and grey literature, following PRISMA guidelines. Studies were included if data was provided on interventions funded across two or more sectors, or multiple budgets. Extracted data were categorised and qualitatively coded.
Results: Of 2751 publications screened, 81 cases of co-financing were identified. Most were from high-income countries (93%), but six innovative models were found in Uganda, Brazil, El Salvador, Mozambique, Zambia, and Kenya that also included non-public and international payers. The highest number of cases involved the health (93%), social care (64%) and education (22%) sectors. Co-financing models were most often implemented with the intention of integrating services across sectors for defined target populations, although models were also found aimed at health promotion activities outside the health sector and cross-sectoral financial rewards. Interventions were either implemented and governed by a single sector or delivered in an integrated manner with cross-sectoral accountability. Resource constraints and political relevance emerged as key enablers of co-financing, while lack of clarity around the roles of different sectoral players and the objectives of the pooling were found to be barriers to success. Although rigorous impact or economic evaluations were scarce, positive process measures were frequently reported with some evidence suggesting co-financing contributed to improved outcomes.
Conclusion: Co-financing remains in an exploratory phase, with diverse models having been implemented across sectors and settings. By incentivising intersectoral action on structural inequities and barriers to health interventions, such a novel financing mechanism could contribute to more effective engagement of non-health sectors; to efficiency gains in the financing of universal health coverage; and to simultaneously achieving health and other well-being related sustainable development goals.
Keywords: Co-financing; Health financing; Intersectoral; Pooled budgets; Social determinants of health.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Stenberg K, Hanssen O, Edejer TT-T, Bertram M, Brindley C, Meshreky A, et al. Financing transformative health systems towards achievement of the health sustainable development goals: a model for projected resource needs in 67 low-income and middle-income countries. Lancet Glob Health. 2017;5:e875–e887. doi: 10.1016/S2214-109X(17)30263-2. - DOI - PMC - PubMed
-
- OECD. The imperative of blended finance. Making Blended Finance Work for the Sustainable Development Goals: OECD; 2018. p. 37–46. Available from: https://www.oecd-ilibrary.org/development/making-blended-finance-work-fo.... Cited 2019 Feb 20
-
- UNDP . Business and the SDGs. 2019.
-
- United Nations Department of Economics and Social Affairs . Addis Ababa Action Agenda: Third International Conference on Financing for Development. 2015.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
