

Repeated episodes of thoracic empyema after spontaneous esophageal rupture
- PMID: 31849387
- PMCID: PMC6892671
- DOI: 10.18999/nagjms.81.4.693
Repeated episodes of thoracic empyema after spontaneous esophageal rupture
Abstract
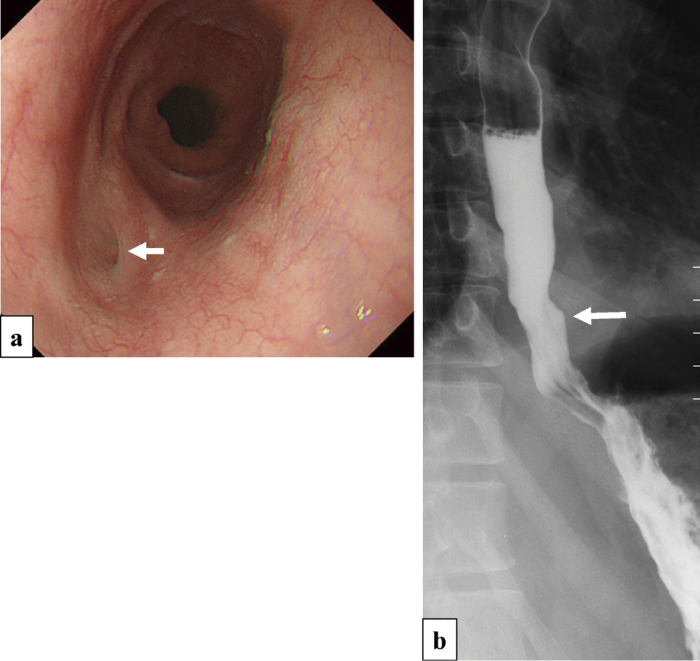
A 52-year-old man with a cough, high fever, and inappetence was diagnosed with thoracic empyema on computed tomography at a local hospital. He had undergone continuous thoracic drainage for a spontaneous esophageal rupture that occurred 17 years earlier. He developed left thoracic empyema 2, 14 and 17 years following the initial esophageal rupture that improved with conservative therapy each time. The most recent episode of thoracic empyema also resolved with conservative therapy. However, he was referred to our hospital for further examination and more complete surgical treatment for recurrent thoracic empyema. Gastrointestinal endoscopy showed a scar from the previous esophageal rupture in the lower esophagus. We considered that recurrent esophageal rupture may have caused repeated episodes of thoracic empyema based on endoscopic findings and his past history and elected to perform subtotal esophagectomy to provide a complete cure. A left transthoracic esophagectomy with a left lower lung lobectomy and gastric tube reconstruction via a retrosternal route were performed. A latissimus dorsi muscle flap was used to eliminate the dead space after lower lung lobectomy to prevent recurrent thoracic empyema. The bronchial stump was covered with a pedicled intercostal muscle flap to prevent leakage from the stump. Minor leakage from the esophagogastrostomy site developed during the postoperative course but resolved with conservative therapy. The patient was transferred to the previous hospital on the 36th postoperative day. Four years after surgery, he had good oral intake and nutritional status without any evidence of recurrent thoracic empyema.
Keywords: spontaneous esophageal rupture; thoracic empyema.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures




References
-
- de Schipper JP, Pull ter Gunne AF, Oostvogel HJ, van Laarhoven CJ. Spontaneous rupture of the oesophagus: Boerhaave's syndrome in 2008. Literature review and treatment algorithm. Dig Surg. 2009;26(1):1–6. - PubMed
-
- Wang SC, Scott WW, Jr. Recurrent spontaneous esophageal rupture managed with esophageal stenting. Ann Thorac Surg. 2016;102(1):e5–6. - PubMed
-
- Ieta K, Oki A, Teshigahara K, et al. Recurrent spontaneous esophageal rupture. Clin J Gastroenterol. 2013;6(1):33–37. - PubMed
-
- D'Journo XB, Doddoli C, Avaro JP, et al. Long-term observation and functional state of the esophagus after primary repair of spontaneous esophageal rupture. Ann Thorac Surg. 2006;81(5):1858–1862. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous