

Clinical Features Predicting Mortality Risk in Patients With Viral Pneumonia: The MuLBSTA Score
- PMID: 31849894
- PMCID: PMC6901688
- DOI: 10.3389/fmicb.2019.02752
Clinical Features Predicting Mortality Risk in Patients With Viral Pneumonia: The MuLBSTA Score
Erratum in
-
Erratum: Clinical Features Predicting Mortality Risk in Patients With Viral Pneumonia: The MuLBSTA Score.Front Microbiol. 2020 Jun 9;11:1304. doi: 10.3389/fmicb.2020.01304. eCollection 2020. Front Microbiol. 2020. PMID: 32582135 Free PMC article.
Abstract
Objective: The aim of this study was to further clarify clinical characteristics and predict mortality risk among patients with viral pneumonia.
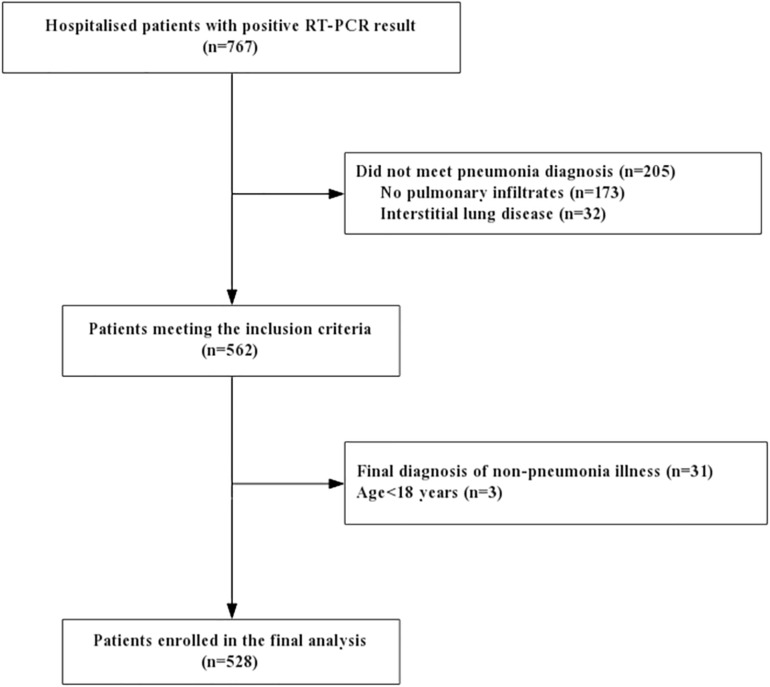
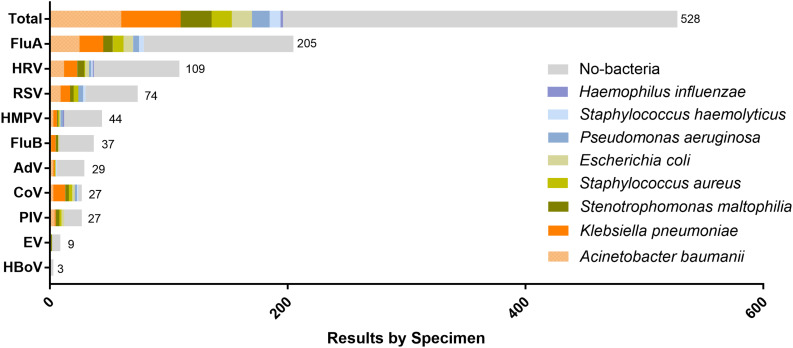
Methods: A total of 528 patients with viral pneumonia at RuiJin hospital in Shanghai from May 2015 to May 2019 were recruited. Multiplex real-time RT-PCR was used to detect respiratory viruses. Demographic information, comorbidities, routine laboratory examinations, immunological indexes, etiological detections, radiological images and treatment were collected on admission.
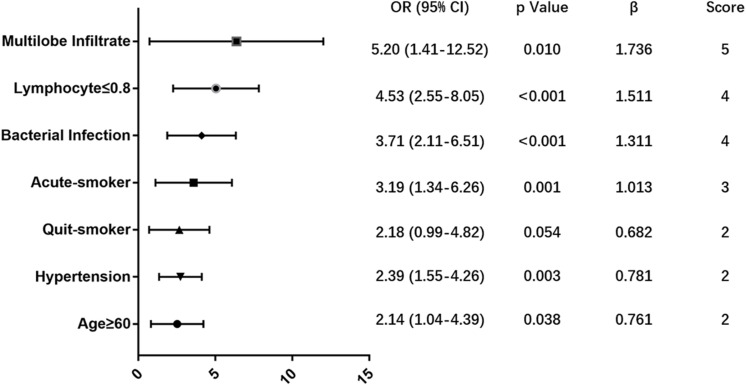
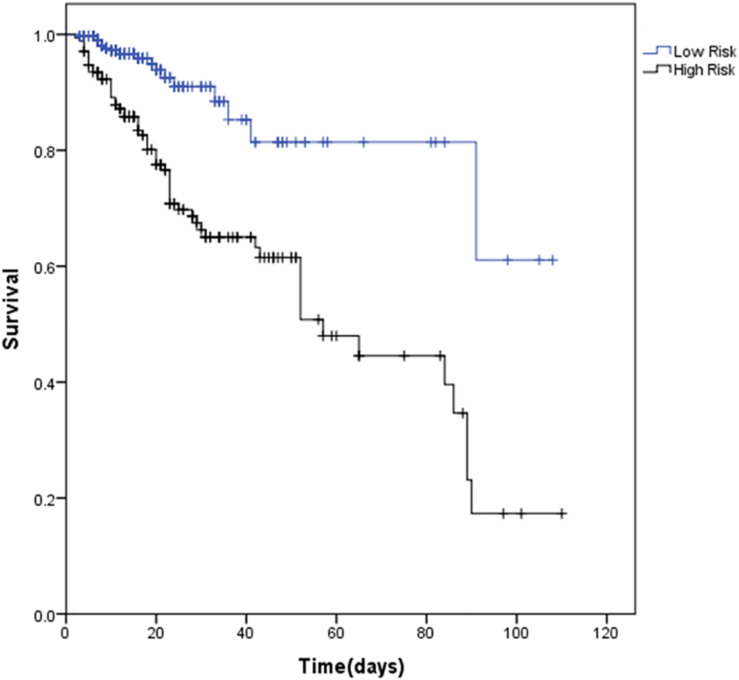
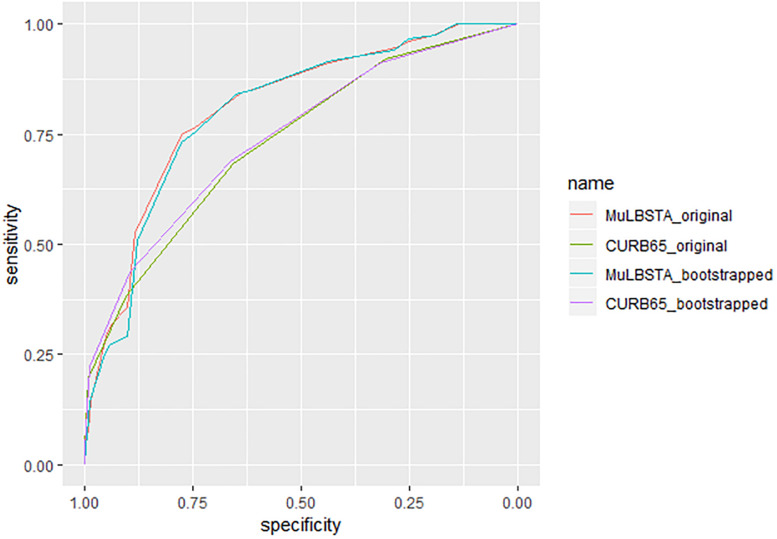
Results: 76 (14.4%) patients died within 90 days in hospital. A predictive MuLBSTA score was calculated on the basis of a multivariate logistic regression model in order to predict mortality with a weighted score that included multilobular infiltrates (OR = 5.20, 95% CI 1.41-12.52, p = 0.010; 5 points), lymphocyte ≤ 0.8∗109/L (OR = 4.53, 95% CI 2.55-8.05, p < 0.001; 4 points), bacterial coinfection (OR = 3.71, 95% CI 2.11-6.51, p < 0.001; 4 points), acute-smoker (OR = 3.19, 95% CI 1.34-6.26, p = 0.001; 3 points), quit-smoker (OR = 2.18, 95% CI 0.99-4.82, p = 0.054; 2 points), hypertension (OR = 2.39, 95% CI 1.55-4.26, p = 0.003; 2 points) and age ≥60 years (OR = 2.14, 95% CI 1.04-4.39, p = 0.038; 2 points). 12 points was used as a cut-off value for mortality risk stratification. This model showed sensitivity of 0.776, specificity of 0.778 and a better predictive ability than CURB-65 (AUROC = 0.773 vs. 0.717, p < 0.001).
Conclusion: Here, we designed an easy-to-use clinically predictive tool for assessing 90-day mortality risk of viral pneumonia. It can accurately stratify hospitalized patients with viral pneumonia into relevant risk categories and could provide guidance to make further clinical decisions.
Keywords: bacterial coinfection; clinical feature; predicting mortality; predictive score model; virus pneumonia.
Copyright © 2019 Guo, Wei, Zhang, Wu, Li, Zhou and Qu.
Figures
References
-
- Bender B. S., Croghan T., Zhang L., Small P. A., Jr. (1992). Transgenic mice lacking class I major histocompatibility complex-restricted T cells have delayed viral clearance and increased mortality after influenza virus challenge. J. Exp. Med. 175 1143–1145. 10.1084/jem.175.4.1143 - DOI - PMC - PubMed
-
- Bjarnason A., Thorleifsdottir G., Löve A., Gudnason J. F., Asgeirsson H., Hallgrimsson K. L., et al. (2012). Severity of influenza A 2009 (H1N1) pneumonia is underestimated by routine prediction rules. Results from a prospective, population-based study. PloS One 7:e46816. 10.1371/journal.pone.0046816 - DOI - PMC - PubMed
-
- Chemaly R. F., Hanmod S. S., Rathod D. B., Ghantoji S. S., Jiang Y., Doshi A., et al. (2012). The characteristics and outcomes of parainfluenza virus infections in 200 patients with leukemia or recipients of hematopoietic stem cell transplantation. Blood 119 2738–2745. 10.1182/blood-2011-08-371112 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical