

Mechanisms of Graft-versus-Host Disease Prevention by Post-transplantation Cyclophosphamide: An Evolving Understanding
- PMID: 31849930
- PMCID: PMC6895959
- DOI: 10.3389/fimmu.2019.02668
Mechanisms of Graft-versus-Host Disease Prevention by Post-transplantation Cyclophosphamide: An Evolving Understanding
Abstract
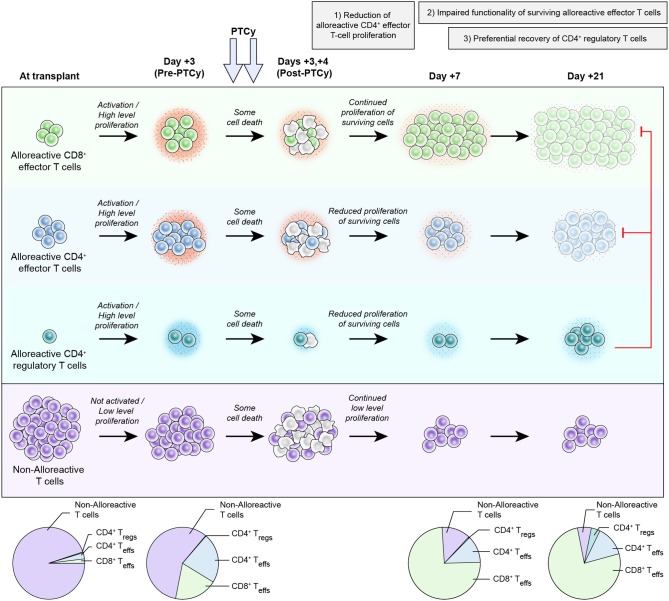
Post-transplantation cyclophosphamide (PTCy) has been highly successful at preventing severe acute and chronic graft-versus-host disease (GVHD) after allogeneic hematopoietic cell transplantation (HCT). The clinical application of this approach was based on extensive studies in major histocompatibility complex (MHC)-matched murine skin allografting models, in which cyclophosphamide was believed to act via three main mechanisms: (1) selective elimination of alloreactive T cells; (2) intrathymic clonal deletion of alloreactive T-cell precursors; and (3) induction of suppressor T cells. In these models, cyclophosphamide was only effective in very specific contexts, requiring particular cell dose, cell source, PTCy dose, and recipient age. Achievement of transient mixed chimerism also was required. Furthermore, these studies showed differences in the impact of cyclophosphamide on transplanted cells (tumor) versus tissue (skin grafts), including the ability of cyclophosphamide to prevent rejection of the former but not the latter after MHC-mismatched transplants. Yet, clinically PTCy has demonstrated efficacy in MHC-matched or partially-MHC-mismatched HCT across a wide array of patients and HCT platforms. Importantly, clinically significant acute GVHD occurs frequently after PTCy, inconsistent with alloreactive T-cell elimination, whereas PTCy is most active against severe acute GVHD and chronic GVHD. These differences between murine skin allografting and clinical HCT suggest that the above-mentioned mechanisms may not be responsible for GVHD prevention by PTCy. Indeed, recent work by our group in murine HCT has shown that PTCy does not eliminate alloreactive T cells nor is the thymus necessary for PTCy's efficacy. Instead, other mechanisms appear to be playing important roles, including: (1) reduction of alloreactive CD4+ effector T-cell proliferation; (2) induced functional impairment of surviving alloreactive CD4+ and CD8+ effector T cells; and (3) preferential recovery of CD4+ regulatory T cells. Herein, we review the history of cyclophosphamide's use in preventing murine skin allograft rejection and our evolving new understanding of the mechanisms underlying its efficacy in preventing GVHD after HCT. Efforts are ongoing to more fully refine and elaborate this proposed new working model. The completion of this effort will provide critical insight relevant for the rational design of novel approaches to improve outcomes for PTCy-treated patients and for the induction of tolerance in other clinical contexts.
Keywords: alloreactive T cells; graft-versus-host disease; haploidentical allogeneic hematopoietic cell transplantation; post-transplantation cyclophosphamide; regulatory T cells; skin allograft rejection; tolerance.
Copyright © 2019 Nunes and Kanakry.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials