

The Impact of Socioeconomic Deprivation on Clinical Outcomes for Pancreatic Adenocarcinoma at a High-volume Cancer Center: A Retrospective Cohort Analysis
- PMID: 31851004
- PMCID: PMC7272283
- DOI: 10.1097/SLA.0000000000003706
The Impact of Socioeconomic Deprivation on Clinical Outcomes for Pancreatic Adenocarcinoma at a High-volume Cancer Center: A Retrospective Cohort Analysis
Abstract
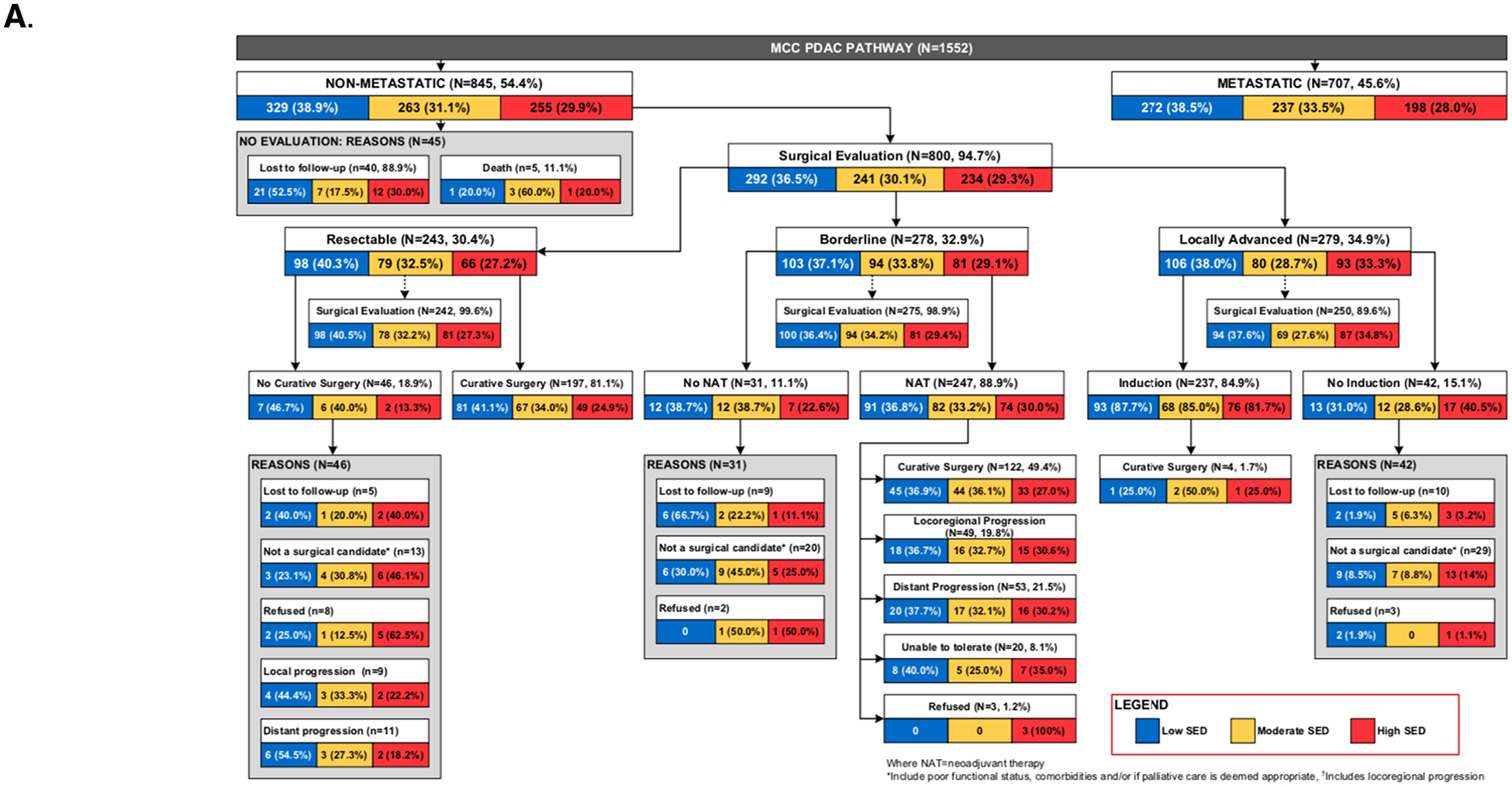
Objective: To assess the impact of a granular measure of SED on pancreatic surgical and cancer-related outcomes at a high-volume cancer center that employs a standardized clinic pathway.
Summary of background data: Prior research has shown that low socioeconomic status leads to less treatment and worse outcomes for PDAC. However, these studies employed inconsistent definitions and categorizations of socioeconomic status, aggregated individual socioeconomic data using large geographic areas, and lacked detailed clinicopathologic variables.
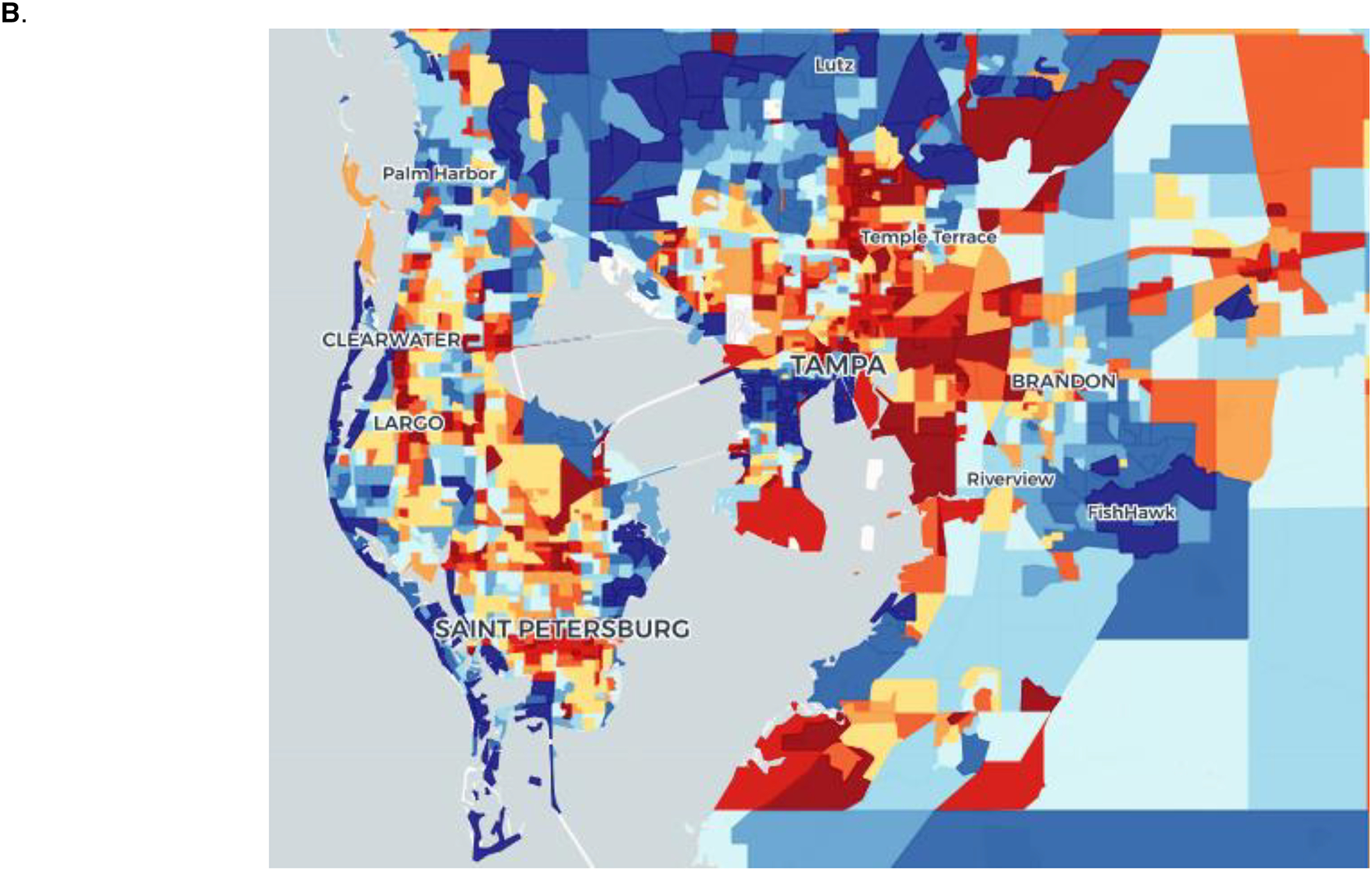
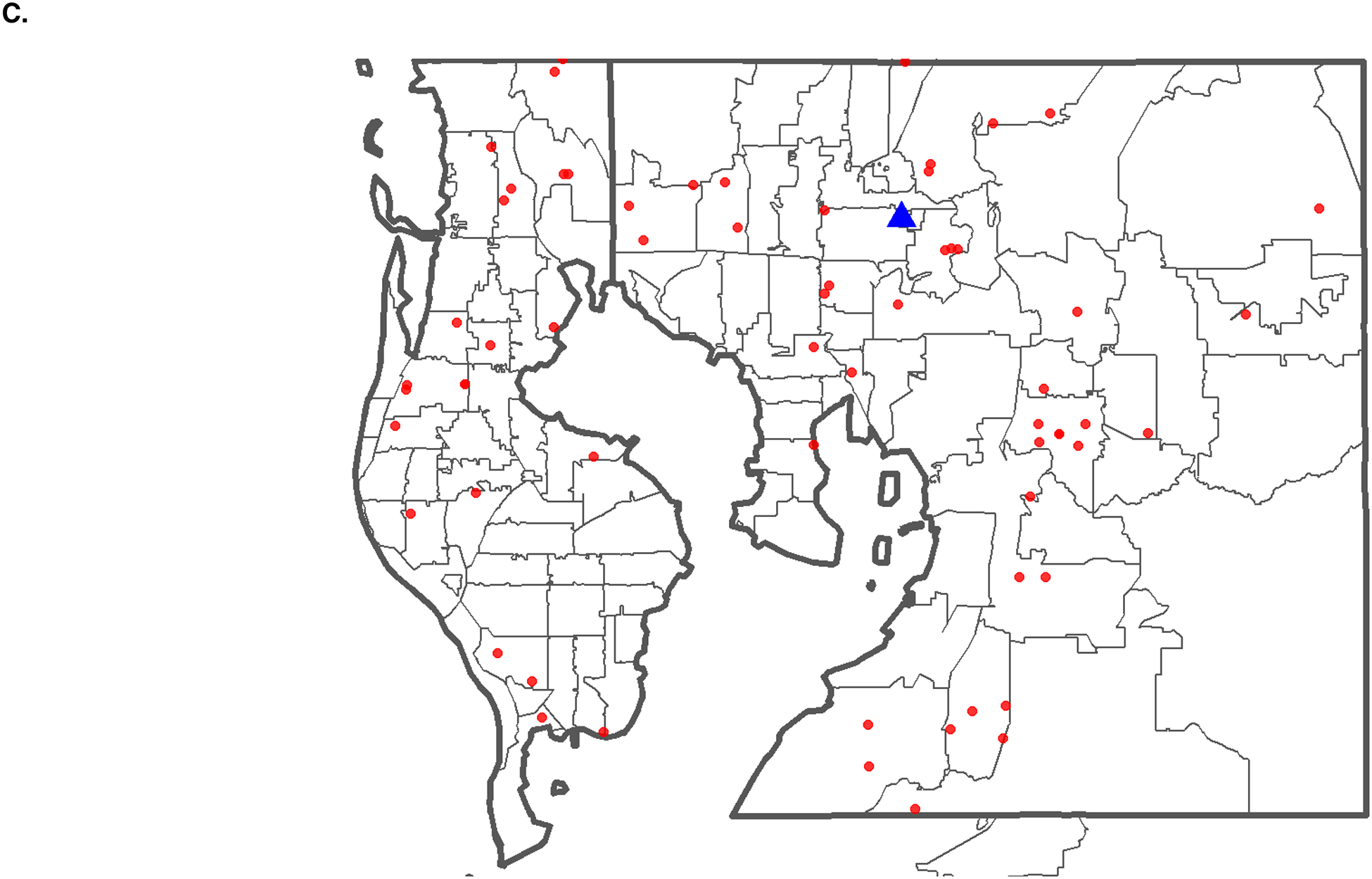
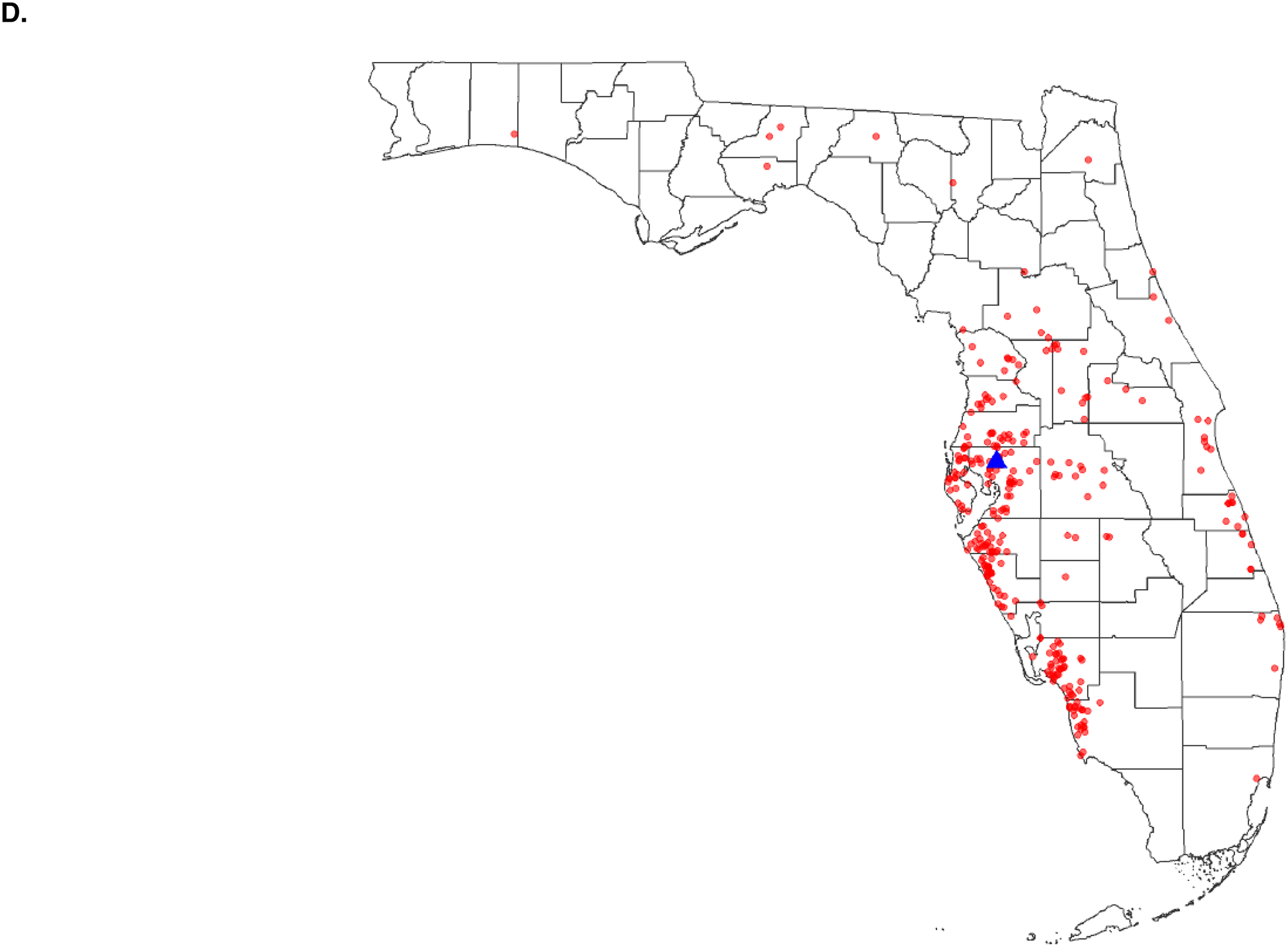
Methods: We conducted a retrospective cohort study of 1552 PDAC patients between 2008 and 2015. Patients were stratified using the area deprivation index, a validated dataset that ranks census block groups based on SED. Multivariable models were used in the curative surgery cohort to predict the impact of SED on (1) grade 3/4 Clavien-Dindo complications, (2) initiation of adjuvant therapy, (3) completion of adjuvant therapy, and (4) overall survival.
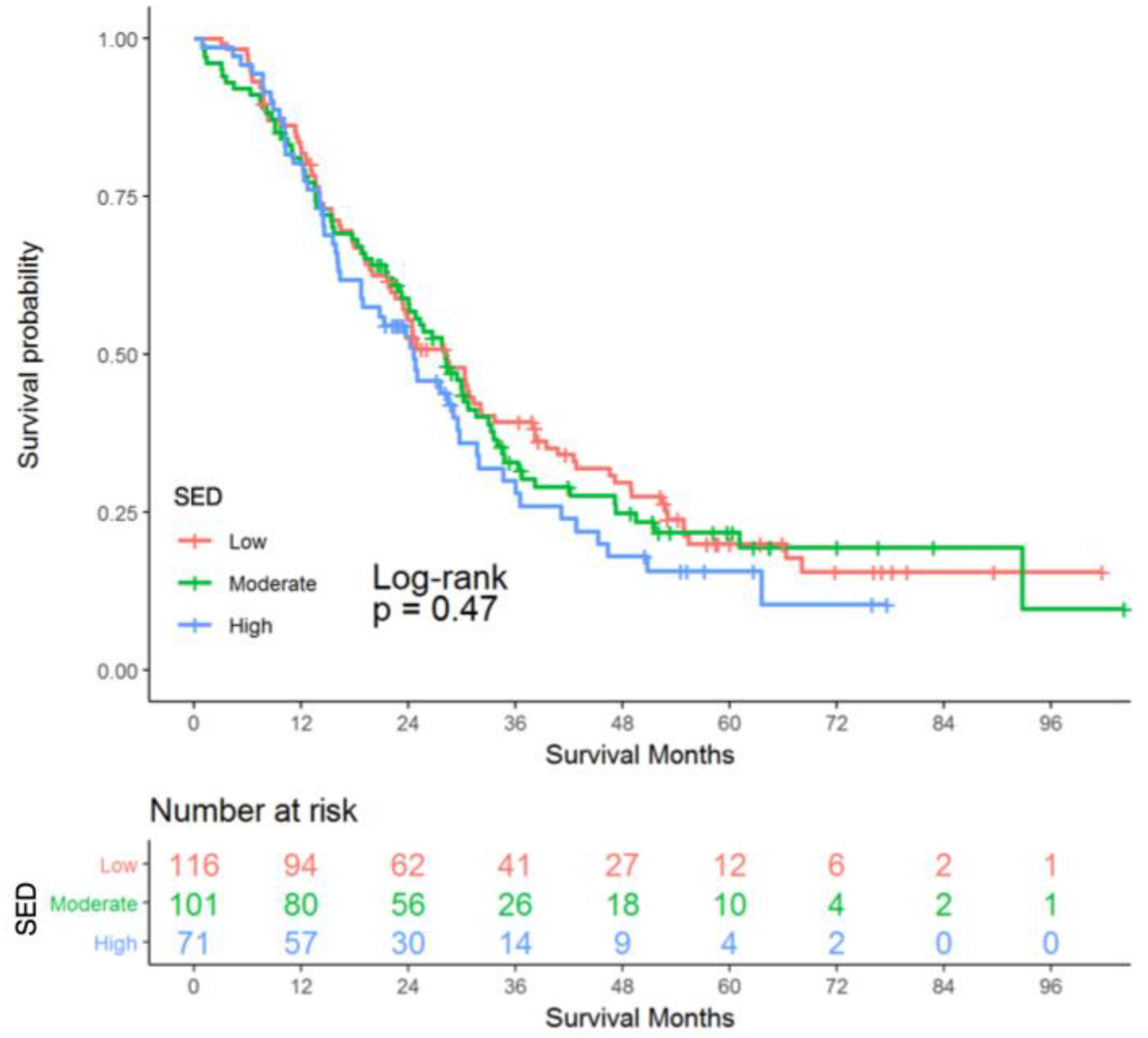
Results: Patients from high SED neighborhoods constituted 29.9% of the cohort. Median overall survival was 28 months. The rate of Clavien-Dindo grade 3/4 complications was 14.2% and completion of adjuvant therapy was 65.6%. There was no evidence that SED impacted surgical evaluation, receipt of curative-intent surgery, postoperative complications, receipt of adjuvant therapy or overall survival.
Conclusions: Although nearly one-quarter of curative-intent surgery patients were from high SED neighborhoods, this factor was not associated with measures of treatment quality or survival. These observations suggest that treatment at a high-volume cancer center employing a standardized clinical pathway may in part address socioeconomic disparities in pancreatic cancer.
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Zell JA, Rhee JM, Ziogas A, et al. Race, socioeconomic status, treatment, and survival time among pancreatic cancer cases in California. Cancer Epidemiol Biomarkers Prev 2007; 16(3):546–52. - PubMed
-
- Moaven O, Richman JS, Reddy S, et al. Healthcare disparities in outcomes of patients with resectable pancreatic cancer. Am J Surg 2018. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
