

Association of Prehospital Plasma Transfusion With Survival in Trauma Patients With Hemorrhagic Shock When Transport Times Are Longer Than 20 Minutes: A Post Hoc Analysis of the PAMPer and COMBAT Clinical Trials
- PMID: 31851290
- PMCID: PMC6990948
- DOI: 10.1001/jamasurg.2019.5085
Association of Prehospital Plasma Transfusion With Survival in Trauma Patients With Hemorrhagic Shock When Transport Times Are Longer Than 20 Minutes: A Post Hoc Analysis of the PAMPer and COMBAT Clinical Trials
Abstract
Importance: Both military and civilian clinical practice guidelines include early plasma transfusion to achieve a plasma to red cell ratio approaching 1:1 to 1:2. However, it was not known how early plasma should be given for optimal benefit. Two recent randomized clinical trials were published, with apparently contradictory results. The Prehospital Air Medical Plasma (PAMPer) clinical trial showed a nearly 30% reduction in mortality with plasma transfusion in the prehospital environment, while the Control of Major Bleeding After Trauma (COMBAT) clinical trial showed no survival improvement.
Objective: To facilitate a post hoc combined analysis of the COMBAT and PAMPer trials to examine questions that could not be answered by either clinical trial alone. We hypothesized that prehospital transport time influenced the effects of prehospital plasma on 28-day mortality.
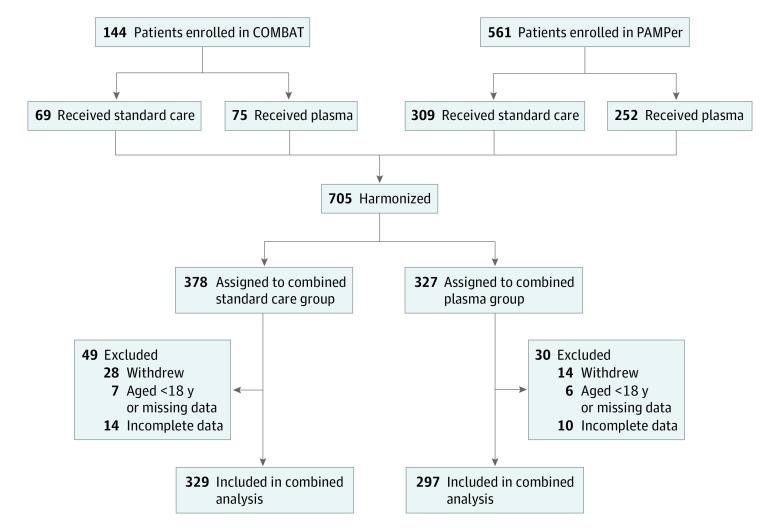
Design, setting, and participants: A total of 626 patients in the 2 clinical trials were included. Patients with trauma and hemorrhagic shock were randomly assigned to receive either standard care or 2 U of thawed plasma followed by standard care in the prehospital environment. Data analysis was performed between September 2018 and January 2019.
Interventions: Prehospital transfusion of 2 U of plasma compared with crystalloid-based resuscitation.
Main outcomes and measures: The main outcome was 28-day mortality.
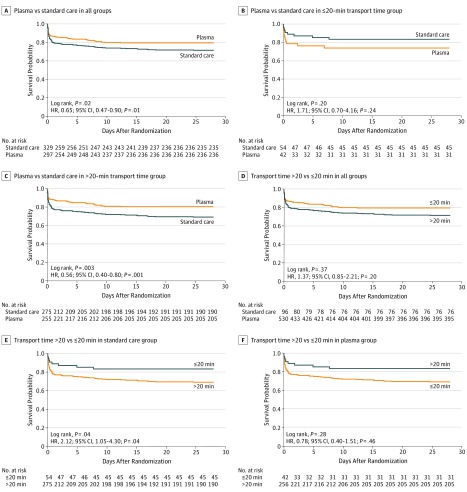
Results: In this post hoc analysis of 626 patients (467 men [74.6%] and 159 women [25.4%]; median [interquartile range] age, 42 [27-57] years) who had trauma with hemorrhagic shock, a Cox regression analysis showed a significant overall survival benefit for plasma (hazard ratio [HR], 0.65; 95% CI, 0.47-0.90; P = .01) after adjustment for injury severity, age, and clinical trial cohort (COMBAT or PAMPer). A significant association with prehospital transport time was detected (from arrival on scene to arrival at the trauma center). Increased mortality was observed in patients in the standard care group when prehospital transport was longer than 20 minutes (HR, 2.12; 95% CI, 1.05-4.30; P = .04), while increased mortality was not observed in patients in the prehospital plasma group (HR, 0.78; 95% CI, 0.40-1.51; P = .46). No serious adverse events were associated with prehospital plasma transfusion.
Conclusions and relevance: These data suggest that prehospital plasma is associated with a survival benefit when transport times are longer than 20 minutes and that the benefit-risk ratio is favorable for use of prehospital plasma.
Trial registration: ClinicalTrials.gov identifiers: NCT01838863 (COMBAT) and NCT01818427 (PAMPer).
Conflict of interest statement
Figures
Comment in
-
Getting Our Money's Worth From Clinical Care Studies of Prehospital Trauma Care.JAMA Surg. 2020 Feb 1;155(2):e195086. doi: 10.1001/jamasurg.2019.5086. Epub 2020 Feb 19. JAMA Surg. 2020. PMID: 31851291 No abstract available.
-
Prehospital Plasma Transfusion and Survival in Trauma Patients With Hemorrhagic Shock.JAMA Surg. 2020 Aug 1;155(8):784. doi: 10.1001/jamasurg.2020.1131. JAMA Surg. 2020. PMID: 32432663 No abstract available.
References
-
- Gurney JM, Spinella PC. Blood transfusion management in the severely bleeding military patient. Curr Opin Anaesthesiol. 2018;31(2):-.https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&li... doi:10.1097/ACO.0000000000000574 - DOI - PubMed
-
- Cannon JW, Khan MA, Raja AS, et al. . Damage control resuscitation in patients with severe traumatic hemorrhage: a practice management guideline from the Eastern Association for the Surgery of Trauma. J Trauma Acute Care Surg. 2017;82(3):605-617.https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&li... doi:10.1097/TA.0000000000001333 - DOI - PubMed
-
- Joint trauma system clinical practice guidelines (CPGs). Department of Defense Center of Excellence for Trauma website. https://jts.amedd.army.mil/index.cfm/PI_CPGs/cpgs. Updated August 6, 2019. Accessed June 12, 2019.
-
- Butler FK, Holcomb JB, Schreiber MA, et al. . Fluid resuscitation for hemorrhagic shock in tactical combat casualty care: TCCC guidelines change 14-01–2 June 2014. J Spec Oper Med. 2014;14(3):13-38. - PubMed
-
- Maegele M, Lefering R, Paffrath T, Tjardes T, Simanski C, Bouillon B; Working Group on Polytrauma of the German Society of Trauma Surgery (DGU) . Red-blood-cell to plasma ratios transfused during massive transfusion are associated with mortality in severe multiple injury: a retrospective analysis from the Trauma Registry of the Deutsche Gesellschaft für Unfallchirurgie. Vox Sang. 2008;95(2):112-119.https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&li... doi:10.1111/j.1423-0410.2008.01074.x - DOI - PubMed
