

Early-Onset Dementia in War Veterans: Brain Polypathology and Clinicopathologic Complexity
- PMID: 31851313
- PMCID: PMC6970453
- DOI: 10.1093/jnen/nlz122
Early-Onset Dementia in War Veterans: Brain Polypathology and Clinicopathologic Complexity
Abstract
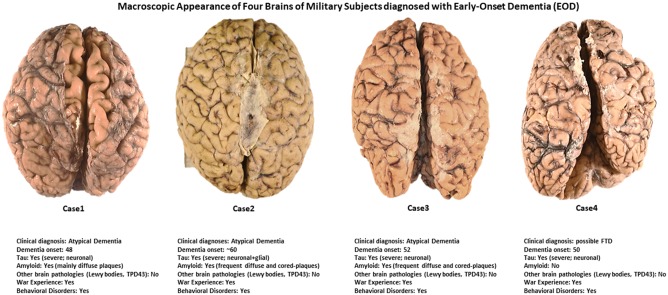
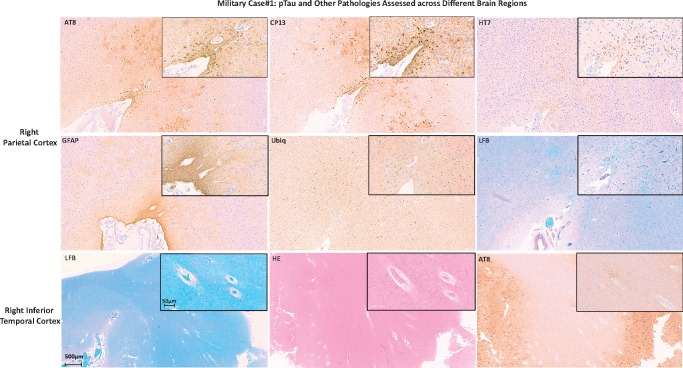
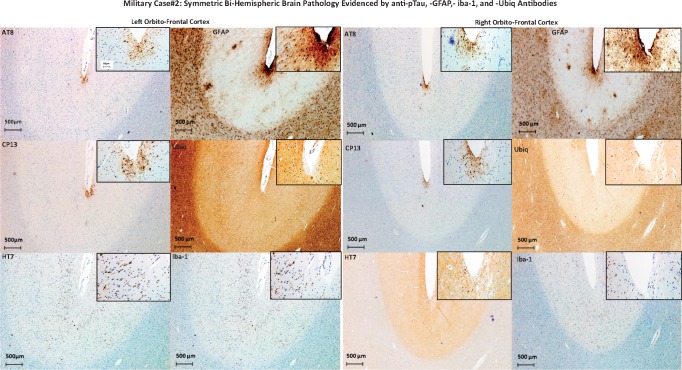
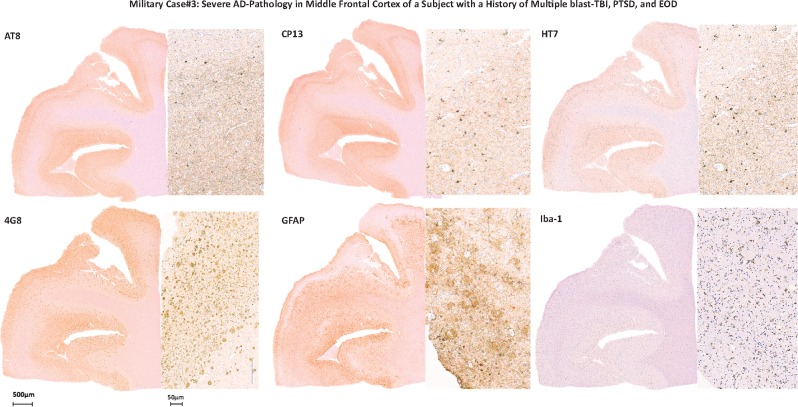
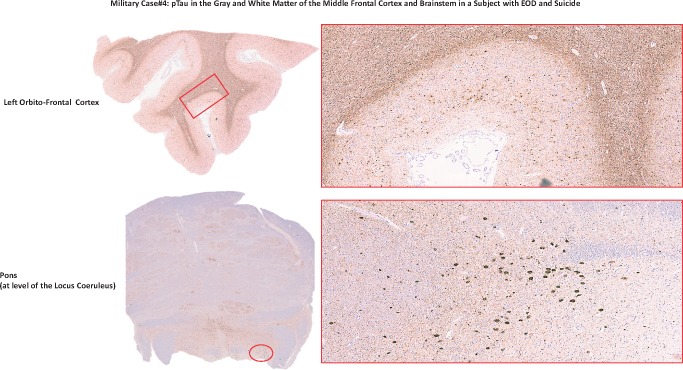
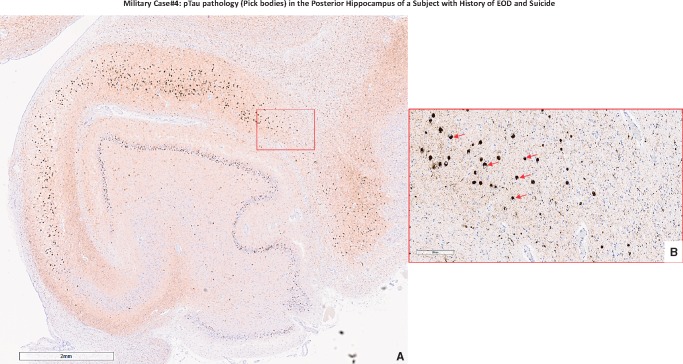
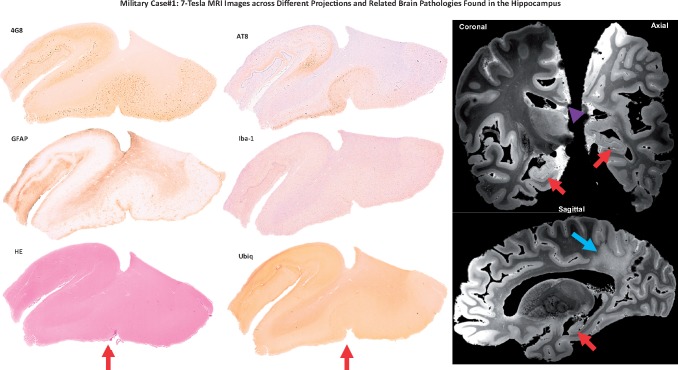
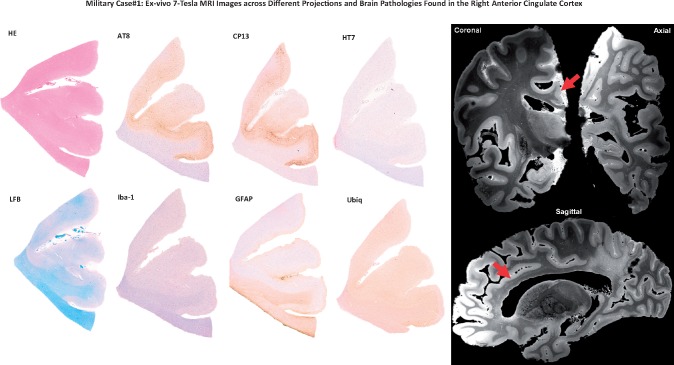
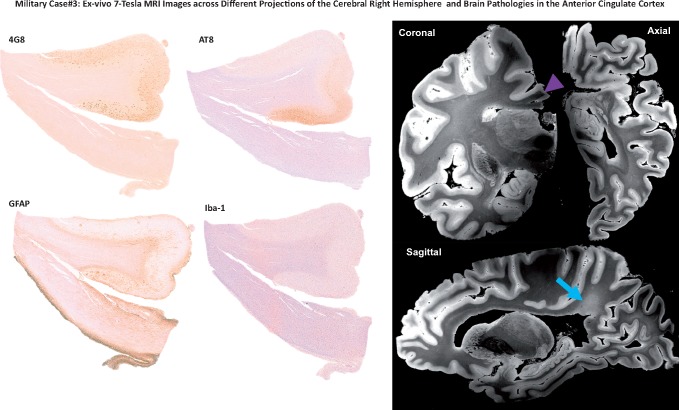
The neuropathology associated with cognitive decline in military personnel exposed to traumatic brain injury (TBI) and chronic stress is incompletely understood. Few studies have examined clinicopathologic correlations between phosphorylated-tau neurofibrillary tangles, β-amyloid neuritic plaques, neuroinflammation, or white matter (WM) lesions, and neuropsychiatric disorders in veterans. We describe clinicopathologic findings in 4 military veterans with early-onset dementia (EOD) who had varying histories of blunt- and blast-TBI, cognitive decline, behavioral abnormalities, post-traumatic stress disorder, suicidal ideation, and suicide. We found that pathologic lesions in these military-EOD cases could not be categorized as classic Alzheimer's disease (AD), chronic traumatic encephalopathy, traumatic axonal injury, or other well-characterized clinicopathologic entities. Rather, we observed a mixture of polypathology with unusual patterns compared with pathologies found in AD or other dementias. Also, ultrahigh resolution ex vivo MRI in 2 of these 4 brains revealed unusual patterns of periventricular WM injury. These findings suggest that military-EOD cases are associated with atypical combinations of brain lesions and distribution rarely seen in nonmilitary populations. Future prospective studies that acquire neuropsychiatric data before and after deployments, as well as genetic and environmental exposure data, are needed to further elucidate clinicopathologic correlations in military-EOD.
Keywords: Brain co-occurring pathologies; Chronic stress; Combat-TBI; Histologic distribution; Short- and long-terms neuropsychiatric manifestations in veterans; War settings.
© 2019 American Association of Neuropathologists, Inc.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
