

Serum Uric Acid Shows Inverted "U" Type Correlation with Osteoporosis in Chinese Ankylosing Spondylitis Patients: A Retrospective Study
- PMID: 31851643
- PMCID: PMC6930702
- DOI: 10.12659/MSM.918766
Serum Uric Acid Shows Inverted "U" Type Correlation with Osteoporosis in Chinese Ankylosing Spondylitis Patients: A Retrospective Study
Abstract
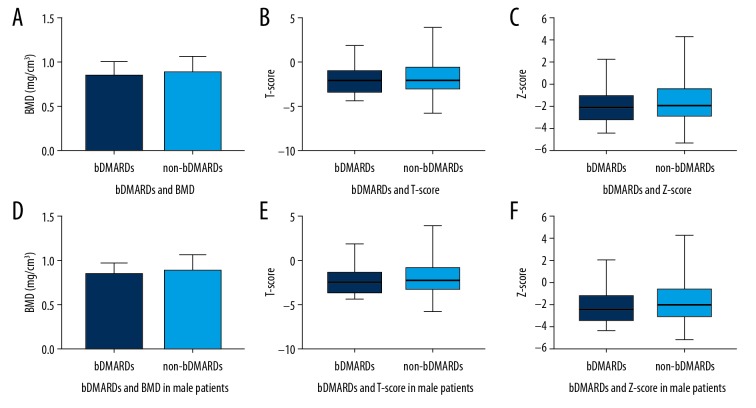
BACKGROUND This study was to investigate the correlation between osteoporosis and serum uric acid in ankylosing spondylitis (AS) patients, and to further identify potential factors that might be associated with osteoporosis in AS patients. MATERIAL AND METHODS We included 182 AS patients, consisted of 143 male patients and 39 female patients, who visited our hospital from January 1, 2014 to December 31, 2018. We used dual-energy x-ray absorptiometry to measure bone mineral density (BMD) of orthotopic lumbar vertebrae in patients with AS. The gender, age, disease duration, BMD, T-score, Z-score, uric acid, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), blood platelet (PLT), and status of treatment with biologics of the patients were collected. Then, the Spearman correlation coefficient and multivariate liner regression analysis were applied to identify the relationship between the factors and BMD, T-score, and Z-score in AS patients. RESULTS Male AS patients between the ages of 16 and 30 years old had a higher risk of osteoporosis (P<0.05). AS patients with uric acid value between 300-360 μmol/L had the highest BMD, T-score, and Z-score. The BMD had a positive correlation with age and disease duration (P<0.01) while had a negative correlation with PLT (P<0.05). BMD in AS patients with elevated ESR was significantly (P<0.05) lower than in AS patients with normal ESR. There were no significant differences in BMD between AS patients with elevated CRP and the patients with normal CRP and PLT. Treatment with TNFi (tumor necrosis factor alpha inhibitor) did not improve BMD in AS patients. CONCLUSIONS The relationship between uric acid and BMD in AS patients was observed as inverted "U"-type. Keeping uric acid within 300-360 μmol/L might be helpful in preventing AS patients from developing osteoporosis.
Conflict of interest statement
None.
Figures






References
-
- Cooper C, Carbone L, Michet CJ, et al. Fracture risk in patients with ankylosing spondylitis: a population-based study. J Rheumatol. 1994;21(10):1877–82. - PubMed
-
- Lee YS, Schlotzhauer T, Ott SM, et al. Skeletal status of men with early and late ankylosing spondylitis. Am J Med. 1997;103(3):233–41. - PubMed
-
- Gao M, Li SL. [Research progress on the relationship between serum uric acid and osteoporosis]. Chinese Journal of Osteoporosis. 2016;22:641–46. [in Chinese]
-
- Kong WP, Zhang W, Tao QW, et al. [Analysis of bone mineral density in 1051 patients with ankylosing spondylitis]. Chinese Journal of Osteoporosis. 2012;18(11):1036–41. [in Chinese]
-
- Vosse D, Landew é R, van der Hejide HD, et al. Ankylosing spondylitis and the risk of fracture: Results from a large primary care-based nested case-control study. Ann Rheum Dis. 2009;68(12):1839–42. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
