

Estimating the global impact of poor quality of care on maternal and neonatal outcomes in 81 low- and middle-income countries: A modeling study
- PMID: 31851685
- PMCID: PMC6919595
- DOI: 10.1371/journal.pmed.1002990
Estimating the global impact of poor quality of care on maternal and neonatal outcomes in 81 low- and middle-income countries: A modeling study
Abstract
Background: In low-resource settings where disease burdens remain high and many health facilities lack essentials such as drugs or commodities, functional equipment, and trained personnel, poor quality of care often results and the impact can be profound. In this paper, we systematically quantify the potential gain of addressing quality of care globally using country-level data about antenatal, childbirth, and postnatal care interventions.
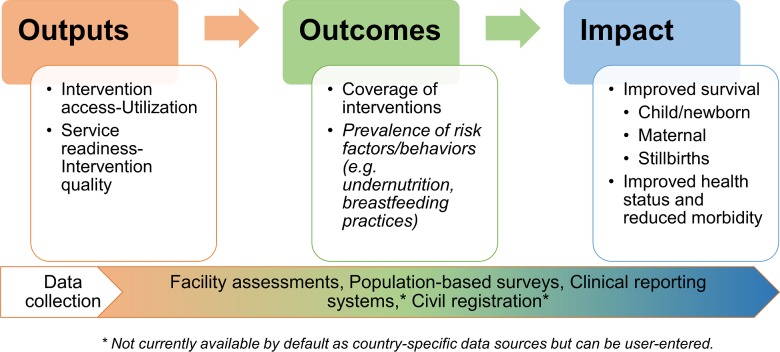
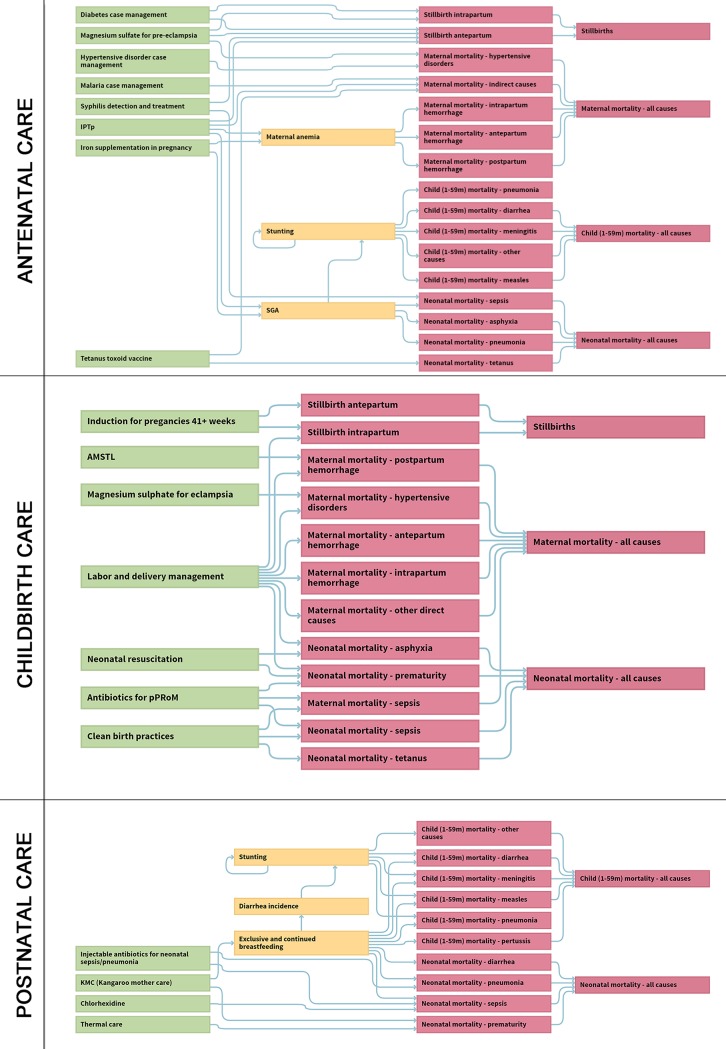
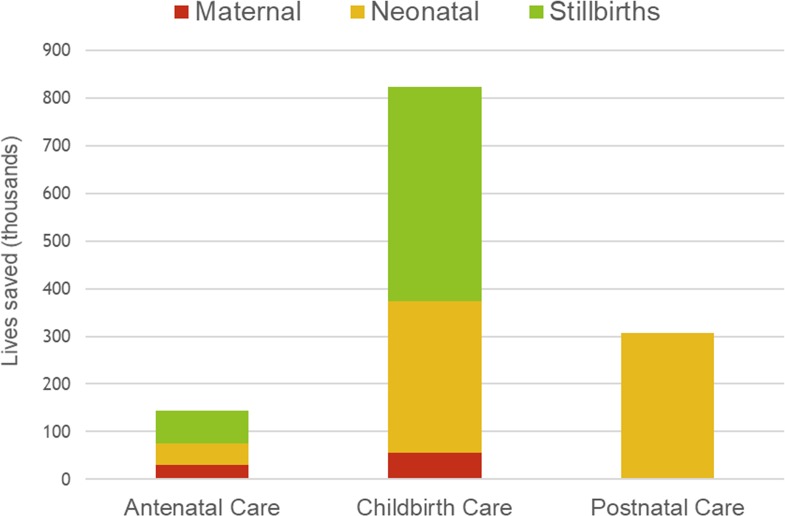
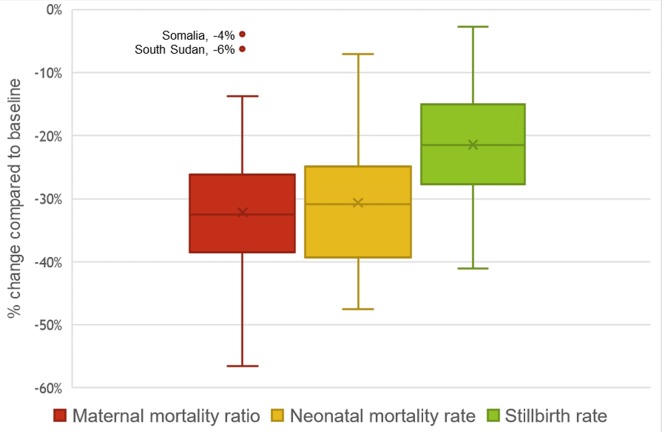
Methods and findings: In this study, we created deterministic models to project health outcomes if quality of care was addressed in a representative sample of 81 low- and middle-income countries (LMICs). First, available data from health facility surveys (e.g., Service Provision Assessment [SPA] and Service Availability and Readiness Assessment [SARA]) conducted 2007-2016 were linked to household surveys (e.g., Demographic and Health Surveys [DHS] and Multiple Indicator Cluster Surveys [MICS]) to estimate baseline coverage for a core subset of 19 maternal and newborn health interventions. Next, models were constructed with the Lives Saved Tool (LiST) using country-specific baseline levels in countries with a linked dataset (n = 17) and sample medians applied as a proxy in countries without linked data. Lastly, these 2016 starting baseline levels were raised to reach targets in 2020 as endline based upon country-specific utilization (e.g., proportion of women who attended 4+ antenatal visits, percentage of births delivered in a health facility) from the latest DHS or MICS population-based reports. Our findings indicate that if high-quality health systems could effectively deliver this subset of evidence-based interventions to mothers and their newborns who are already seeking care, there would be an estimated 28% decrease in maternal deaths, 28% decrease in neonatal deaths, and 22% fewer stillbirths compared to a scenario without any change or improvement in quality of care. Totals of 86,000 (range, 77,800-92,400) maternal and 0.67 million (range, 0.59 million-0.75 million) neonatal lives could be saved, and 0.52 million (range, 0.48 million-0.55 million) stillbirths could be prevented across the 81 countries in the calendar year 2020 when adequate quality care is provided at current levels of utilization. Limitations include the paucity of data to individually assess quality of care for each intervention in all LMICs and the necessary assumption that quality of care being provided among the subset of countries with linked datasets is comparable or representative of LMICs overall.
Conclusions: Our findings suggest that efforts to close the quality gap would still produce substantial benefits at current levels of access or utilization. With estimated mortality rate declines of 21%-32% on average, gains from this first step would be significant if quality was improved for selected antenatal, intrapartum, and postnatal interventions to benefit pregnant women and newborns seeking care. Interventions provided at or around the time of childbirth are most critical and accounted for 64% of the impact overall estimated in this quality improvement analysis.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- World Health Organization. Everybody business: strengthening health systems to improve health outcomes: WHO’s framework for action. Geneva; 2007.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
