

Effectiveness and cost-effectiveness of home-based postpartum care on neonatal mortality and exclusive breastfeeding practice in low-and-middle-income countries: a systematic review and meta-analysis
- PMID: 31852432
- PMCID: PMC6921506
- DOI: 10.1186/s12884-019-2651-6
Effectiveness and cost-effectiveness of home-based postpartum care on neonatal mortality and exclusive breastfeeding practice in low-and-middle-income countries: a systematic review and meta-analysis
Abstract
Background: Early postpartum facility discharge negatively impacts mothers' proper and effective use postnatal care. Cognizant of these facts, home-based postnatal care practices have been promoted to complement facility-based care to reduce neonatal mortality. This systematic review evaluated the effectiveness and cost-effectiveness of home-based postnatal care on exclusive breastfeeding practice and neonatal mortality in low-and-middle-income countries.
Methods: Randomized trials and quasi-experimental studies were searched from electronic databases including PubMed, Popline, Cochrane Central Register of Controlled Trials and National Health Service Economic Evaluation databases. Random-effects meta-analysis model was used to pool the estimates of the outcomes accounting for the variability among studies.
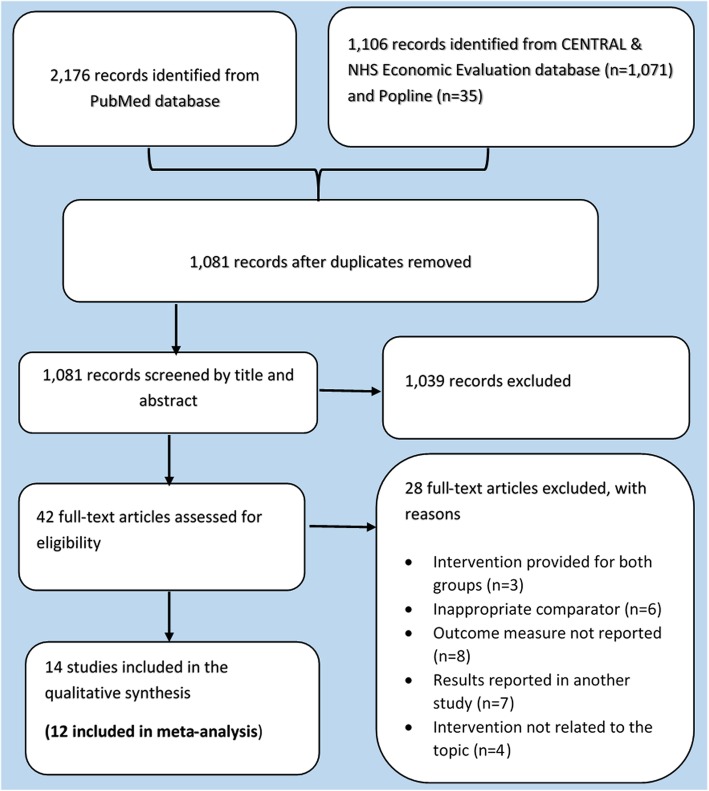
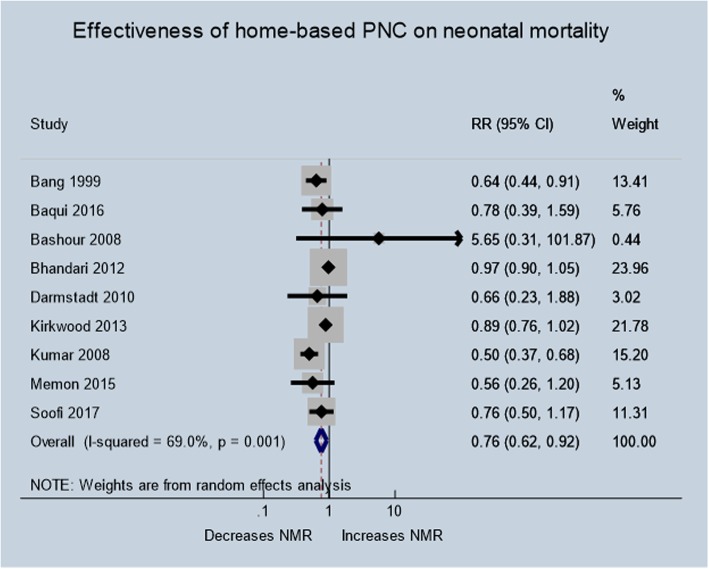
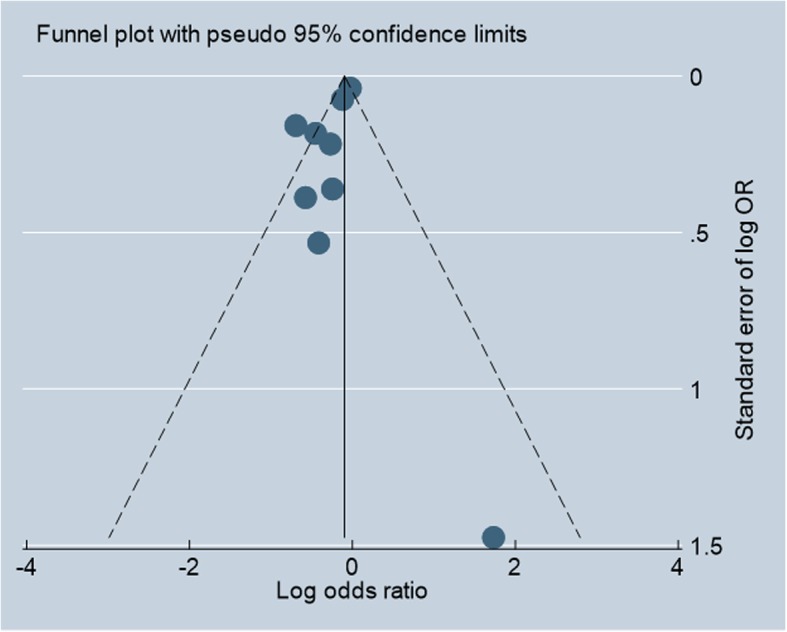
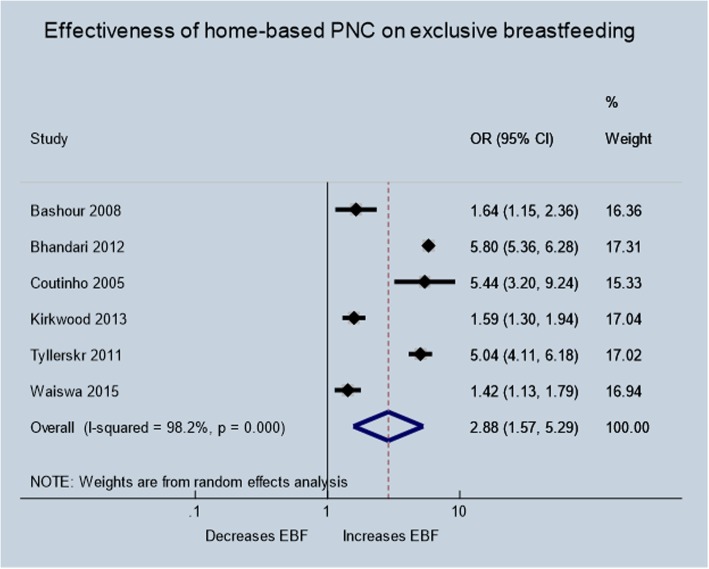
Results: We identified 14 trials implementing intervention packages that included preventive and promotive newborn care services, home-based treatment for sick neonates, and community mobilization activities. The pooled analysis indicates that home-based postpartum care reduced neonatal mortally by 24% (risk ratio 0.76; 95% confidence interval 0.62-0.92; 9 trials; n = 93,083; heterogeneity p < .01) with no evidence of publication bias (Egger's test: Coef. = - 1.263; p = .130). The subgroup analysis suggested that frequent home visits, home visits by community health workers, and community mobilization efforts with home visits, to had better neonatal survival. Likewise, the odds of mothers who exclusively breastfed from the home visit group were about three times higher than the mothers who were in the routine care group (odds ratio: 2.88; 95% confidence interval: 1.57-5.29; 6 trials; n = 20,624 mothers; heterogeneity p < .01), with low possibility of publication bias (Coef. = - 7.870; p = .164). According to the World Health Organization's Choosing Interventions that are Cost-Effective project recommendations, home-based neonatal care strategy was found to be cost-effective.
Conclusions: Home visits and community mobilization activities to promote neonatal care practices by community health workers is associated with reduced neonatal mortality, increased practice of exclusive breastfeeding, and cost-effective in improving newborn health outcomes for low-and-middle-income countries. However, a well-designed evaluation study is required to formulate the optimal package and optimal timing of home visits to standardize home-based postnatal interventions.
Keywords: Cost; Cost-effectiveness; Exclusive breastfeeding; Home visit; Home-based newborn care; Home-based postnatal care; Low-and-middle-income countries; Neonatal mortality; Postpartum home visit.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Lawn JE, Cousens S, Zupan J. 4 million neonatal deaths: when? Where? Why? Lancet 2005;365(9462):891–900. doi:https://doi.org/10.1016/S0140-6736(05)71048-5. - PubMed
-
- Bhutta ZA, Das JK, Bahl R, Lawn JE, Salam RA, Paul VK et al. Can available interventions end preventable deaths in mothers, newborn babies, and stillbirths, and at what cost? Lancet 2014;384(9940):347–370. doi:https://doi.org/10.1016/S0140-6736(14)60792-3. - PubMed
-
- WHO, UNICEF, UNFPA, World Bank Group, United Nations population division . Trends in maternal mortality: 1990 to 2015 population and development review. Geneva: World Health Organization; 2015.
