

The double burden of malnutrition: aetiological pathways and consequences for health
- PMID: 31852605
- PMCID: PMC7613491
- DOI: 10.1016/S0140-6736(19)32472-9
The double burden of malnutrition: aetiological pathways and consequences for health
Abstract
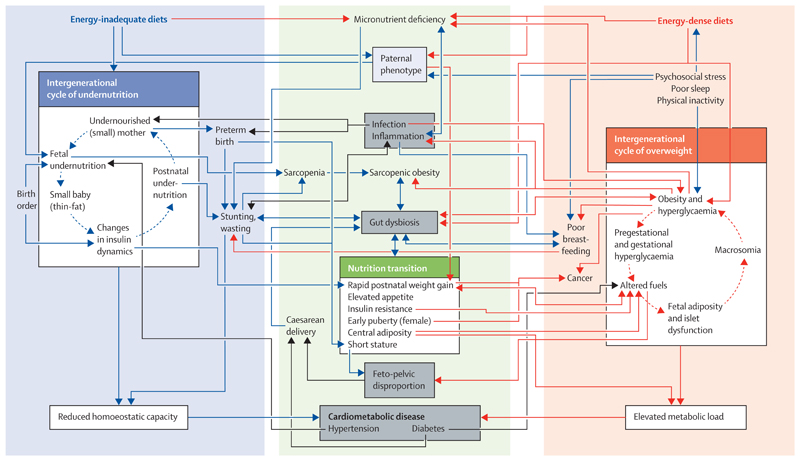
Malnutrition has historically been researched and addressed within two distinct silos, focusing either on undernutrition, food insecurity, and micronutrient deficiencies, or on overweight, obesity, and dietary excess. However, through rapid global nutrition transition, an increasing proportion of individuals are exposed to different forms of malnutrition during the life course and have the double burden of malnutrition (DBM) directly. Long-lasting effects of malnutrition in early life can be attributed to interconnected biological pathways, involving imbalance of the gut microbiome, inflammation, metabolic dysregulation, and impaired insulin signalling. Life-course exposure to early undernutrition followed by later overweight increases the risk of non-communicable disease, by imposing a high metabolic load on a depleted capacity for homoeostasis, and in women increases the risk of childbirth complications. These life-course trajectories are shaped both by societal driving factors-ie, rapidly changing diets, norms of eating, and physical activity patterns-and by broader ecological factors such as pathogen burden and extrinsic mortality risk. Mitigation of the DBM will require major societal shifts regarding nutrition and public health, to implement comprehensive change that is sustained over decades, and scaled up into the entire global food system.
Copyright © 2020 World Health Organization. Published by Elsevier Ltd. All rights reserved. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
We declare no competing interests.
Figures
Comment in
-
A new nutrition manifesto for a new nutrition reality.Lancet. 2020 Jan 4;395(10217):8-10. doi: 10.1016/S0140-6736(19)32690-X. Epub 2019 Dec 15. Lancet. 2020. PMID: 31852600 No abstract available.
-
A future direction for tackling malnutrition.Lancet. 2020 Jan 4;395(10217):2. doi: 10.1016/S0140-6736(19)33099-5. Epub 2019 Dec 15. Lancet. 2020. PMID: 31852604 No abstract available.
References
-
- Doak CM, Adair LS, Bentley M, Monteiro C, Popkin BM. The dual burden household and the nutrition transition paradox. IntJ Obes (Lond) 2005;29:129–36. - PubMed
-
- Swinburn BA, Kraak VI, Allender S, et al. The global syndemic of obesity, undernutrition, and climate change: the Lancet Commission report. Lancet. 2019;393:791–846. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
