

Intergroup Randomized Phase III Study of Postoperative Oxaliplatin, 5-Fluorouracil, and Leucovorin Versus Oxaliplatin, 5-Fluorouracil, Leucovorin, and Bevacizumab for Patients with Stage II or III Rectal Cancer Receiving Preoperative Chemoradiation: A Trial of the ECOG-ACRIN Research Group (E5204)
- PMID: 31852811
- PMCID: PMC7216434
- DOI: 10.1634/theoncologist.2019-0437
Intergroup Randomized Phase III Study of Postoperative Oxaliplatin, 5-Fluorouracil, and Leucovorin Versus Oxaliplatin, 5-Fluorouracil, Leucovorin, and Bevacizumab for Patients with Stage II or III Rectal Cancer Receiving Preoperative Chemoradiation: A Trial of the ECOG-ACRIN Research Group (E5204)
Abstract
Background: The addition of bevacizumab to chemotherapy improved outcomes for patients with metastatic colon cancer. E5204 was designed to test whether the addition of bevacizumab to mFOLFOX6, following neoadjuvant chemoradiation and definitive surgery, could improve overall survival (OS) in patients with stage II/III adenocarcinoma of the rectum.
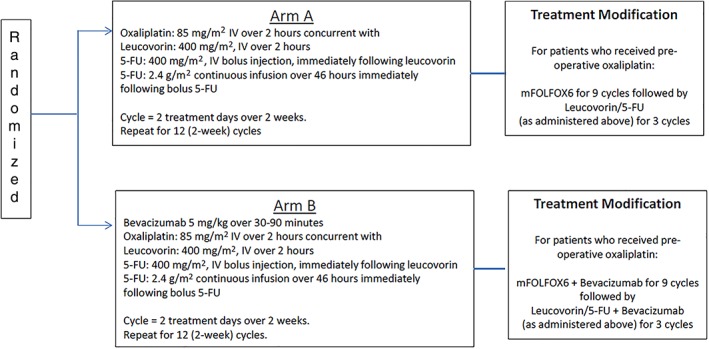
Subjects, materials, and methods: Patients with stage II/III rectal cancer who had completed neoadjuvant 5-fluorouracil-based chemoradiation and had undergone complete resection were enrolled. Patients were randomized to mFOLFOX6 (Arm A) or mFOLFOX6 with bevacizumab (Arm B) administered every 2 weeks for 12 cycles.
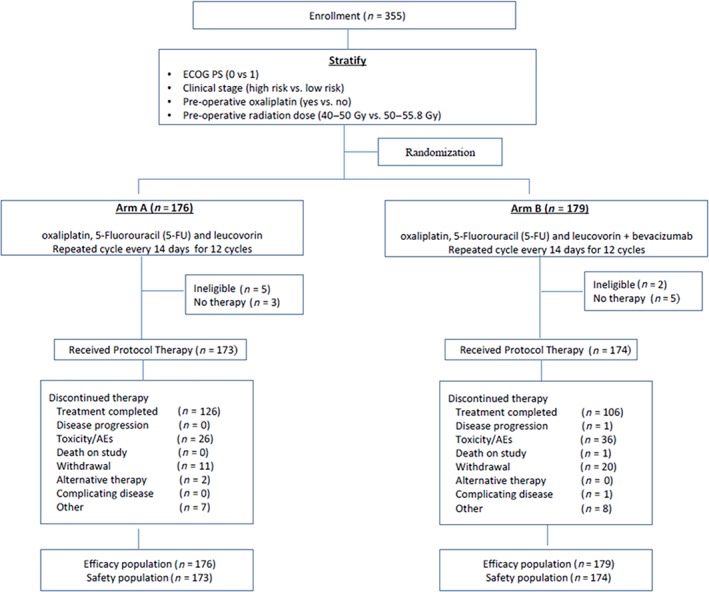
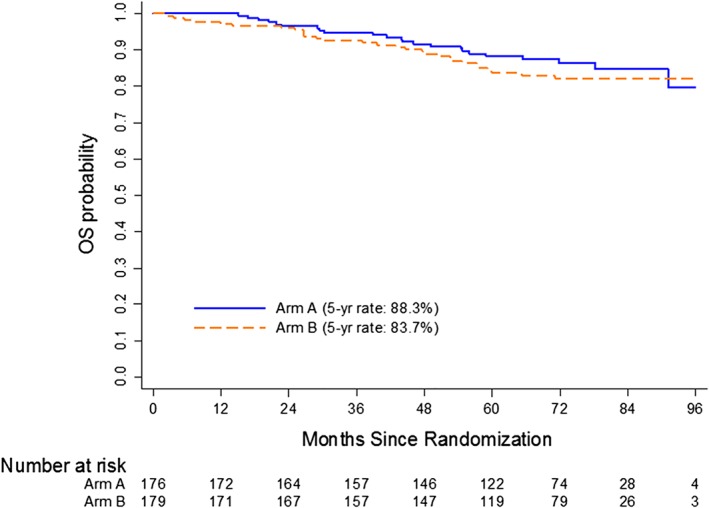
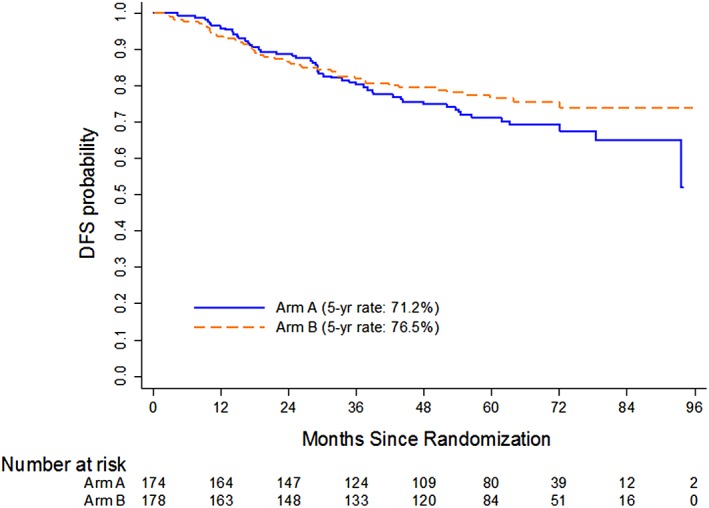
Results: E5204 registered only 355 patients (17% of planned accrual goal) as it was terminated prematurely owing to poor accrual. At a median follow-up of 72 months, there was no difference in 5-year overall survival (88.3% vs. 83.7%) or 5-year disease-free survival (71.2% vs. 76.5%) between the two arms. The rate of treatment-related grade ≥ 3 adverse events (AEs) was 68.8% on Arm A and 70.7% on Arm B. Arm B had a higher proportion of patients who discontinued therapy early as a result of AEs and patient withdrawal than did Arm A (32.4% vs. 21.5%, p = .029).The most common grade 3-4 treatment-related AEs were neutropenia, leukopenia, neuropathy, diarrhea (without prior colostomy), and fatigue.
Conclusion: At 17% of its planned accrual, E5204 did not meet its primary endpoint. The addition of bevacizumab to FOLFOX6 in the adjuvant setting did not significantly improve OS in patients with stage II/III rectal cancer.
Implications for practice: At 17% of its planned accrual, E5204 was terminated early owing to poor accrual. At a median follow-up of 72 months, there was no significant difference in 5-year overall survival (88.3% vs. 83.7%) or in 5-year disease-free survival (71.2% vs. 76.5%) between the two arms. Despite significant advances in the treatment of rectal cancer, especially in improving local control rates, the risk of distant metastases and the need to further improve quality of life remain a challenge. Strategies combining novel agents with chemoradiation to improve both distant and local control are needed.
Keywords: Adjuvant therapy; Antiangiogenesis; Avastin; Bevacizumab; Rectal cancer.
© AlphaMed Press 2019.
Conflict of interest statement
Figures
References
-
- Sauer R, Liersch T, Merkel S et al. Preoperative versus postoperative chemoradiotherapy for locally advanced rectal cancer: Results of the German CAO/ARO/AIO‐94 randomized phase III trial after a median follow‐up of 11 years. J Clin Oncol 2012;30:1926–1933. - PubMed
-
- André T, Boni C, Mounedji‐Boudiaf L et al. Oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment for colon cancer. N Engl J Med 2004;350:2343–2351. - PubMed
-
- Kuebler JP, Wieand HS, O'Connell MJ et al. Oxaliplatin combined with weekly bolus fluorouracil and leucovorin as surgical adjuvant chemotherapy for stage II and III colon cancer: Results from NSABP C‐07. J Clin Oncol 2007;25:2198–2204. - PubMed
-
- Benson AB, Catalano P, Meropol NJ et al. ECOG E3201: Intergroup randomized phase III study of postoperative irinotecan, 5‐ fluorouracil (FU), leucovorin (LV) (FOLFIRI) vs oxaliplatin, FU/LV (FOLFOX) vs FU/LV for patients (pts) with stage II/ III rectal cancer receiving either pre or postoperative radiation (RT)/ FU. J Clin Oncol 2006;24(suppl 18):3526.
-
- Hurwitz H, Fehrenbacher L, Novotny W et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med 2004;350:2335–2342. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U10 CA180868/CA/NCI NIH HHS/United States
- UG1 CA189867/CA/NCI NIH HHS/United States
- U10 CA180821/CA/NCI NIH HHS/United States
- UG1 CA189858/CA/NCI NIH HHS/United States
- U10 CA180847/CA/NCI NIH HHS/United States
- UG1 CA189863/CA/NCI NIH HHS/United States
- U10 CA180818/CA/NCI NIH HHS/United States
- UG1 CA189819/CA/NCI NIH HHS/United States
- U10 CA180820/CA/NCI NIH HHS/United States
- U10 CA180794/CA/NCI NIH HHS/United States
- U10 CA180888/CA/NCI NIH HHS/United States
- U10 CA180858/CA/NCI NIH HHS/United States
- UG1 CA189872/CA/NCI NIH HHS/United States
- UG1 CA189828/CA/NCI NIH HHS/United States
- UG1 CA233373/CA/NCI NIH HHS/United States
- U10 CA180863/CA/NCI NIH HHS/United States
- U10 CA180790/CA/NCI NIH HHS/United States
- U10 CA180867/CA/NCI NIH HHS/United States
- U10 CA180838/CA/NCI NIH HHS/United States
- U10 CA180853/CA/NCI NIH HHS/United States
- U10 CA180844/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
