

Targeting liver stage malaria with metformin
- PMID: 31852843
- PMCID: PMC6975259
- DOI: 10.1172/jci.insight.127441
Targeting liver stage malaria with metformin
Abstract
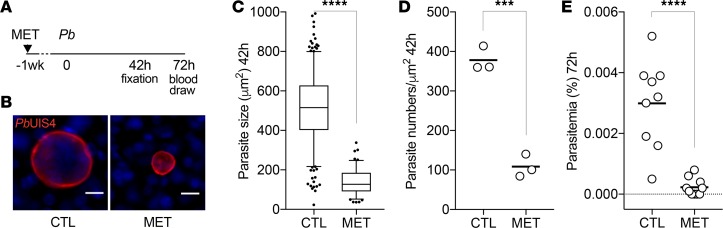
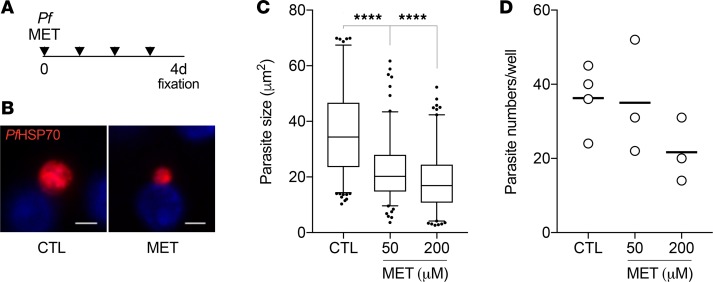
Despite an unprecedented 2 decades of success, the combat against malaria - the mosquito-transmitted disease caused by Plasmodium parasites - is no longer progressing. Efforts toward eradication are threatened by the lack of an effective vaccine and a rise in antiparasite drug resistance. Alternative approaches are urgently needed. Repurposing of available, approved drugs with distinct modes of action are being considered as viable and immediate adjuncts to standard antimicrobial treatment. Such strategies may be well suited to the obligatory and clinically silent first phase of Plasmodium infection, where massive parasite replication occurs within hepatocytes in the liver. Here, we report that the widely used antidiabetic drug, metformin, impairs parasite liver stage development of both rodent-infecting Plasmodium berghei and human-infecting P. falciparum parasites. Prophylactic treatment with metformin curtails parasite intracellular growth in vitro. An additional effect was observed in mice with a decrease in the numbers of infected hepatocytes. Moreover, metformin provided in combination with conventional liver- or blood-acting antimalarial drugs further reduced the total burden of P. berghei infection and substantially lessened disease severity in mice. Together, our findings indicate that repurposing of metformin in a prophylactic regimen could be considered for malaria chemoprevention.
Keywords: Drug therapy; Infectious disease; Malaria; Microbiology; Parasitology.
Conflict of interest statement
Figures

References
-
- World Health Organization. World Malaria Report 2010. http://www.who.int/malaria/world_malaria_report_2010/en/index.html Accessed November 18, 2019.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
