

Intruding implements: a pictorial review of retained surgical foreign objects in neuroradiology
- PMID: 31853666
- PMCID: PMC6920316
- DOI: 10.1186/s13244-019-0817-4
Intruding implements: a pictorial review of retained surgical foreign objects in neuroradiology
Abstract
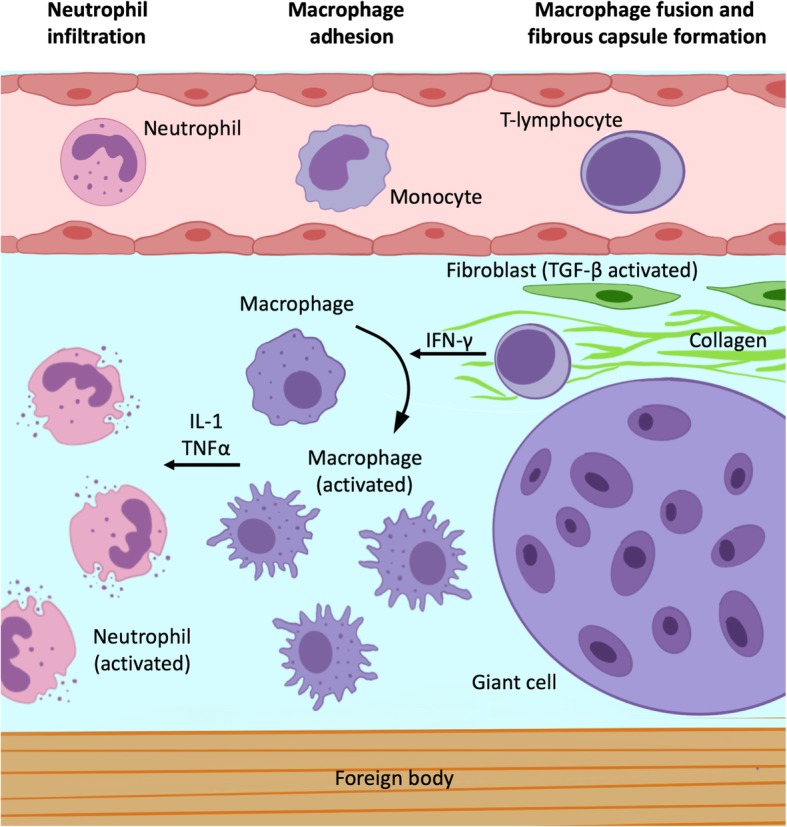
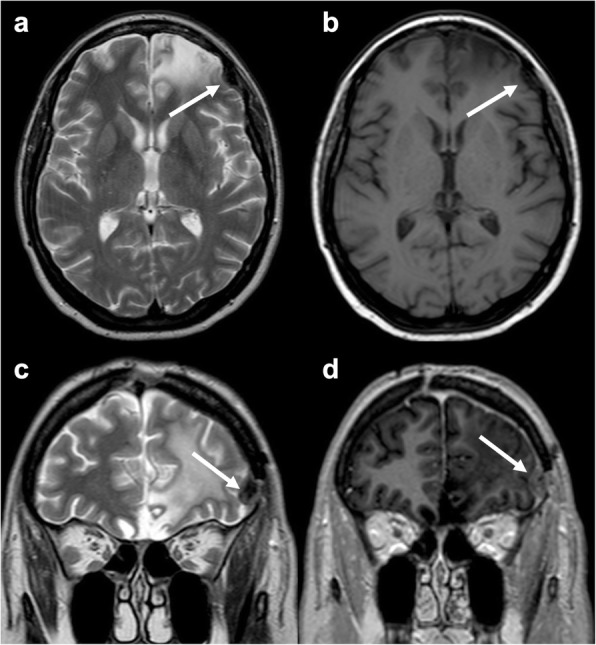
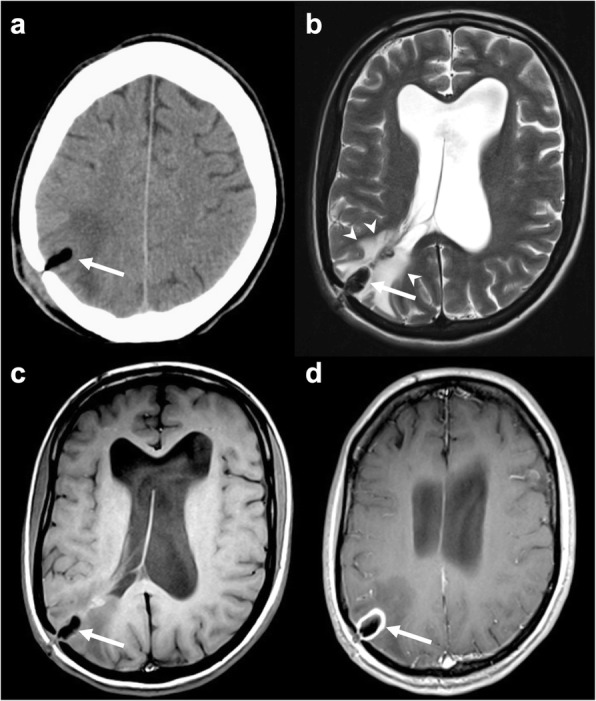
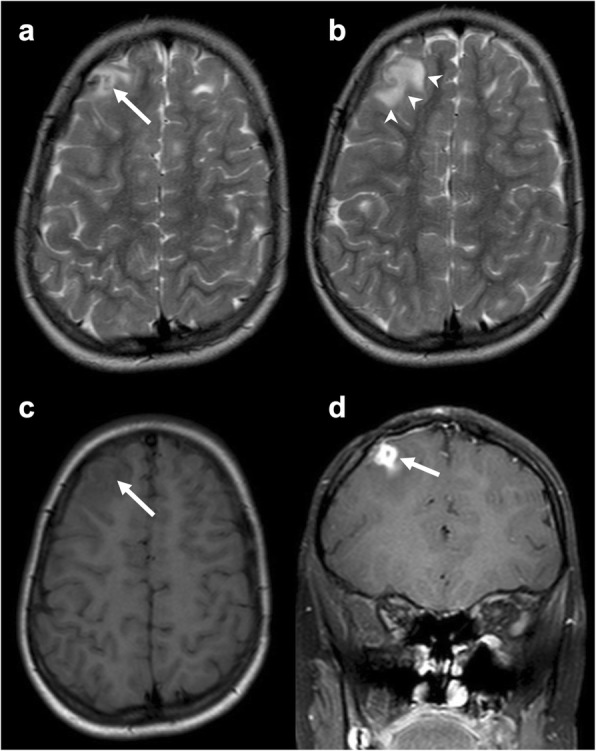
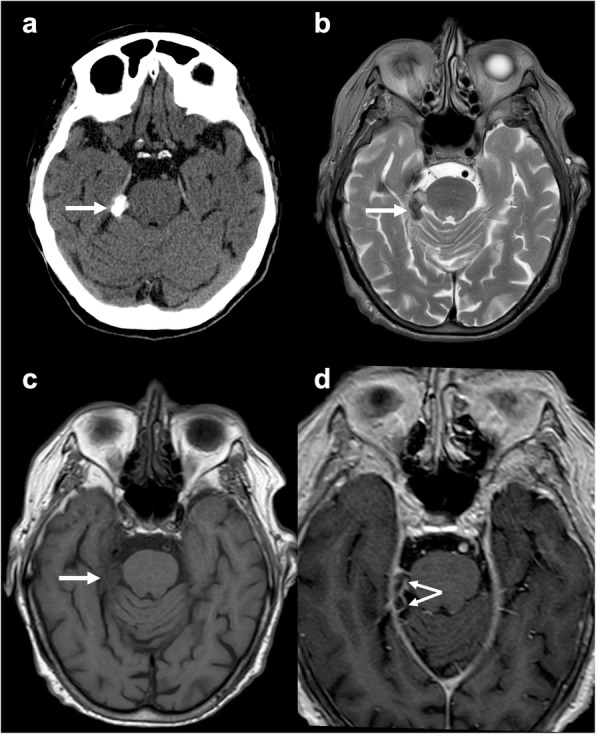
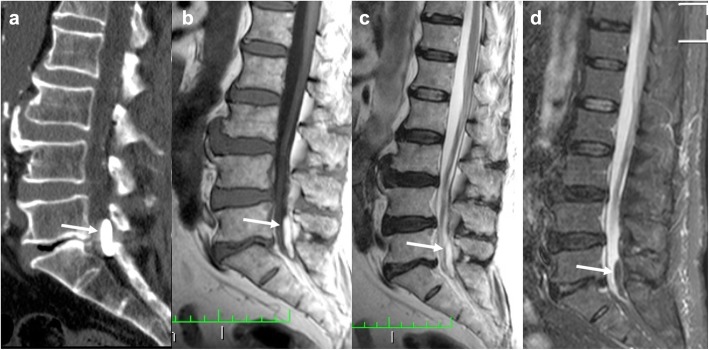
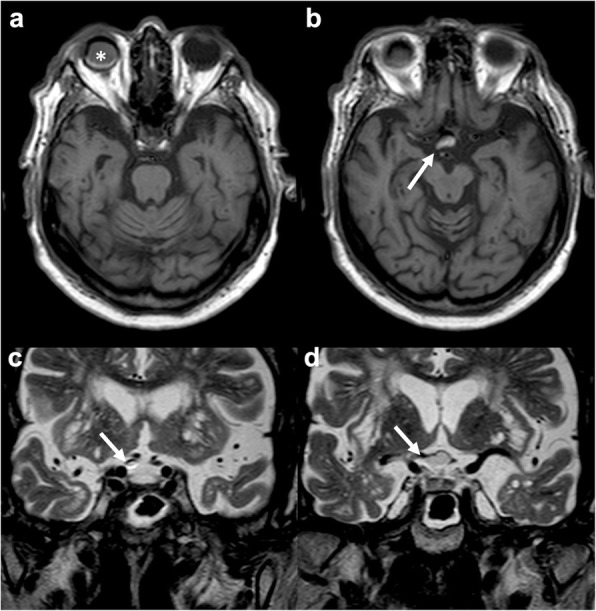
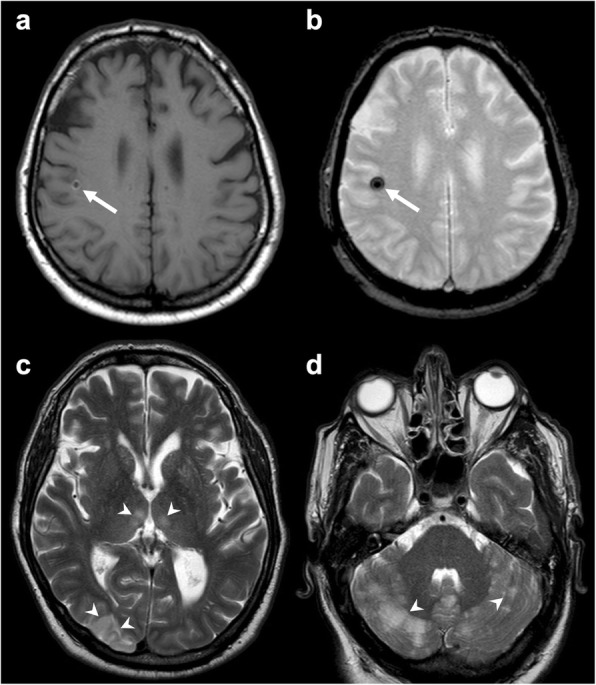
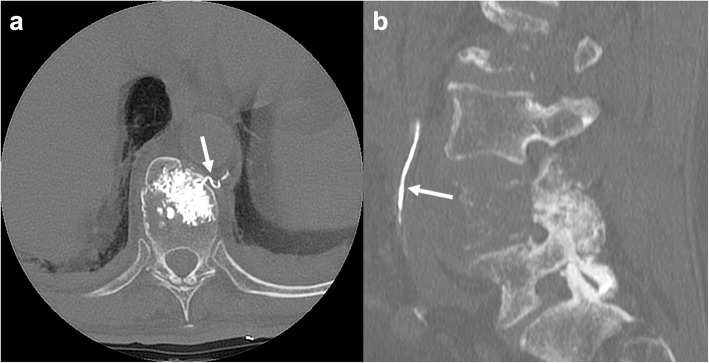
Intra-cranial and spinal foreign body reactions represent potential complications of medical procedures. Their diagnosis may be challenging as they frequently show an insidious clinical presentation and can mimic other life-threatening conditions. Their pathophysiological mechanism is represented by a local inflammatory response due to retained or migrated surgical elements. Cranial interventions may be responsible for the presence of retained foreign objects represented by surgical materials (such as sponges, bone wax, and Teflon). Spinal diagnostic and therapeutic procedures, including myelography, chordotomy, vertebroplasty, and device implantation, are another potential source of foreign bodies. These reactions can also follow material migration or embolization, for example in the case of Lipiodol, Teflon, and cement vertebroplasty. Imaging exams, especially CT and MRI, have a central role in the differential diagnosis of these conditions together with patient history. Neuroradiological findings are dependent on the type of material that has been left in or migrated from the surgical area. Knowledge of these entities is relevant for clinical practice as the correct identification of foreign bodies and related inflammatory reactions, material embolisms, or migrations can be difficult. This pictorial review reports neuroradiological semeiotics and differential diagnosis of foreign body-related imaging abnormalities in the brain and spine.
Keywords: Brain; Computed tomography; Foreign bodies; Magnetic resonance imaging; Spine.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
Publication types
LinkOut - more resources
Full Text Sources
