

Sex, Gender, and Sex Hormones in Pulmonary Hypertension and Right Ventricular Failure
- PMID: 31853950
- PMCID: PMC7338988
- DOI: 10.1002/cphy.c190011
Sex, Gender, and Sex Hormones in Pulmonary Hypertension and Right Ventricular Failure
Abstract
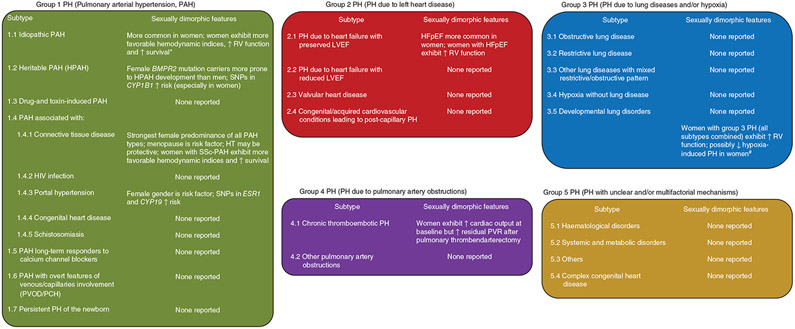
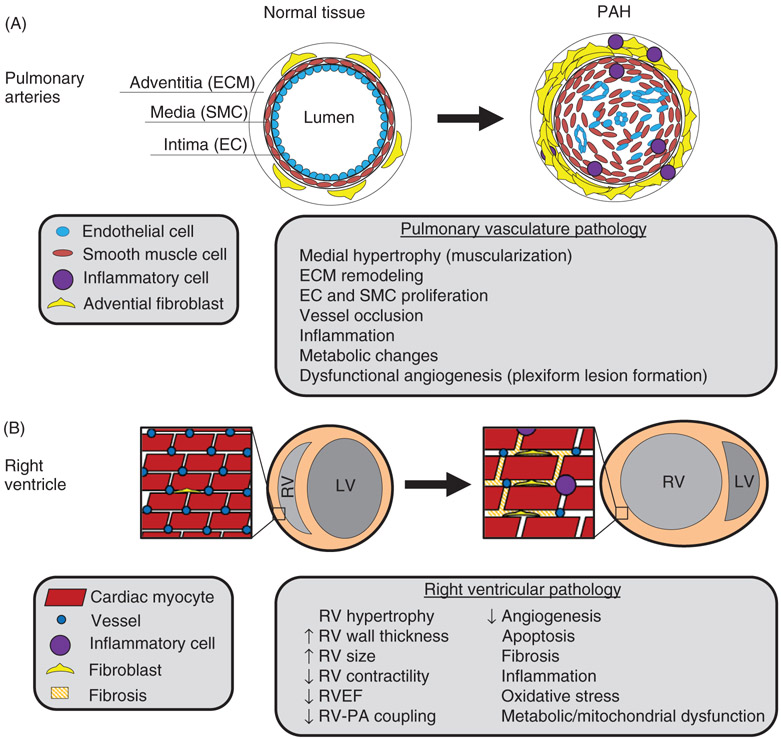
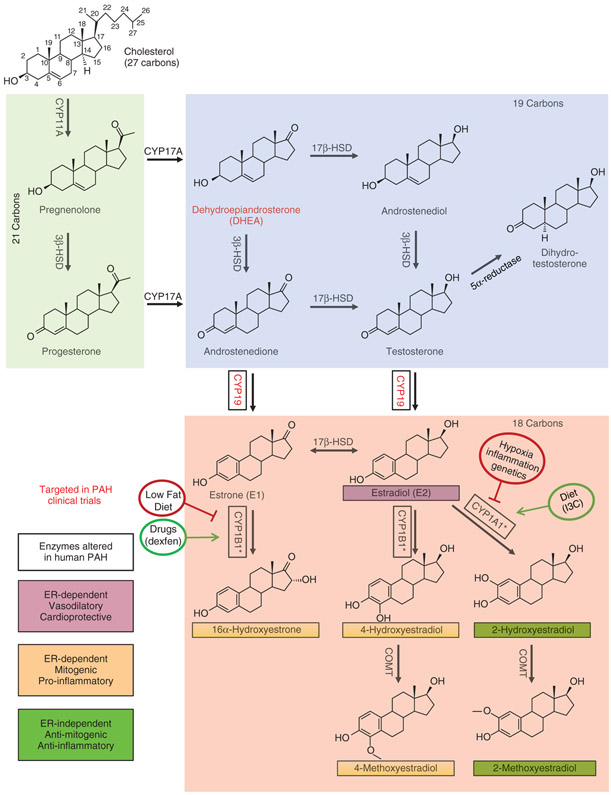
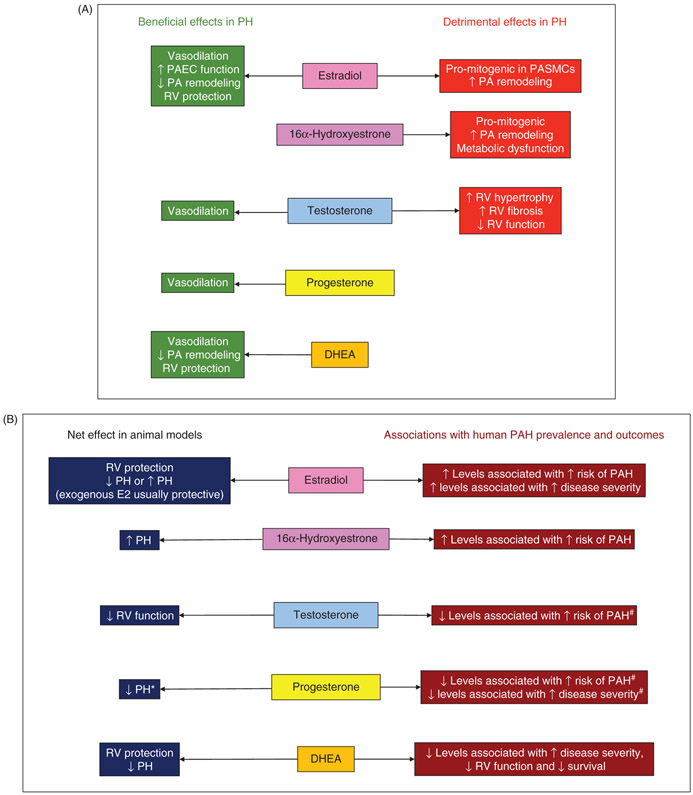
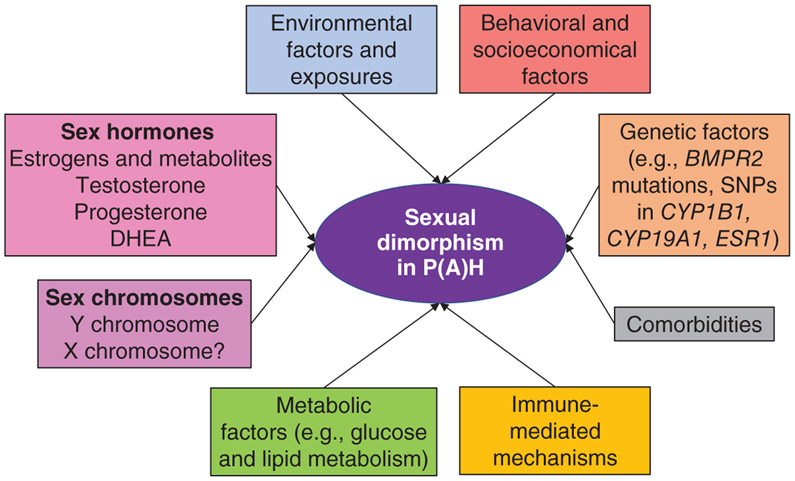
Pulmonary hypertension (PH) encompasses a syndrome of diseases that are characterized by elevated pulmonary artery pressure and pulmonary vascular remodeling and that frequently lead to right ventricular (RV) failure and death. Several types of PH exhibit sexually dimorphic features in disease penetrance, presentation, and progression. Most sexually dimorphic features in PH have been described in pulmonary arterial hypertension (PAH), a devastating and progressive pulmonary vasculopathy with a 3-year survival rate <60%. While patient registries show that women are more susceptible to development of PAH, female PAH patients display better RV function and increased survival compared to their male counterparts, a phenomenon referred to as the "estrogen paradox" or "estrogen puzzle" of PAH. Recent advances in the field have demonstrated that multiple sex hormones, receptors, and metabolites play a role in the estrogen puzzle and that the effects of hormone signaling may be time and compartment specific. While the underlying physiological mechanisms are complex, unraveling the estrogen puzzle may reveal novel therapeutic strategies to treat and reverse the effects of PAH/PH. In this article, we (i) review PH classification and pathophysiology; (ii) discuss sex/gender differences observed in patients and animal models; (iii) review sex hormone synthesis and metabolism; (iv) review in detail the scientific literature of sex hormone signaling in PAH/PH, particularly estrogen-, testosterone-, progesterone-, and dehydroepiandrosterone (DHEA)-mediated effects in the pulmonary vasculature and RV; (v) discuss hormone-independent variables contributing to sexually dimorphic disease presentation; and (vi) identify knowledge gaps and pathways forward. © 2020 American Physiological Society. Compr Physiol 10:125-170, 2020.
Copyright © 2019 American Physiological Society. All rights reserved.
Figures
References
-
- Abenhaim L, Moride Y, Brenot F, Rich S, Benichou J, Kurz X, Higenbottam T, Oakley C, Wouters E, Aubier M, Simonneau G, Begaud B. Appetite-suppressant drugs and the risk of primary pulmonary hypertension. International Primary Pulmonary Hypertension Study Group. N Engl J Med 335: 609–616, 1996. - PubMed
-
- Albrecht ED, Pepe GJ. Placental steroid hormone biosynthesis in primate pregnancy. Endocr Rev 11 (1): 124–150, 1990. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
