

The Role of Maintenance Strategies in Metastatic Colorectal Cancer: A Systematic Review and Network Meta-analysis of Randomized Clinical Trials
- PMID: 31855256
- PMCID: PMC6990730
- DOI: 10.1001/jamaoncol.2019.4489
The Role of Maintenance Strategies in Metastatic Colorectal Cancer: A Systematic Review and Network Meta-analysis of Randomized Clinical Trials
Abstract
Importance: In metastatic colorectal cancer, induction combination chemotherapy with a targeted agent is considered the mainstay of treatment. Multiple randomized clinical trials have examined different strategies of continuing cytotoxic therapy until progression compared with a period of either observation or the use of various maintenance agents. However, those randomized clinical trials have shown inconsistent efficacy results that make it challenging to draw any conclusion on which strategy is preferred. Therefore, a network meta-analysis is helpful to compare different agents across randomized clinical trials.
Objective: To evaluate the comparative effectiveness of different treatment strategies for patients with metastatic colorectal cancer.
Evidence review: MEDLINE, Embase, Scopus, Web of Science, and the Cochrane Central Register of Controlled Trials were searched for randomized clinical trials evaluating different strategies for patients with previously untreated metastatic colorectal cancer. Trials of interest included those including patients with metastatic colorectal cancer who were treated with an initial period of cytotoxic chemotherapy (with or without a biologic) and then switched to one of the following strategies: observation; maintenance with bevacizumab (Bev), fluoropyrimidine (FP), or both (FP + Bev); or continuing the induction regimen until progression. Outcomes of interest included overall survival (OS) and progression-free survival (PFS). The overall effect was pooled using the DerSimonian and Laird random-effects model. Network meta-analysis was conducted using a random-effects consistency model to pool evidence from direct and indirect comparisons. Agents were ranked using surface under the cumulative ranking (SUCRA) probabilities. Higher SUCRA scores correspond to greater efficacy. Initial analysis was performed on December 18, 2018. An updated search was performed in April 2019, and no additional studies were added.
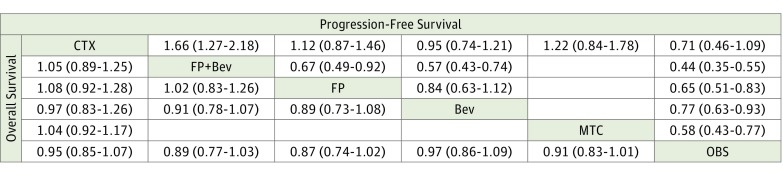
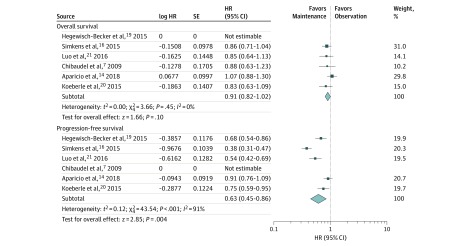
Findings: Twelve trials at low risk of bias (5540 patients; age range, 23-85 years; 64.4 % male) were included. Network meta-analysis showed no benefit of continuing full cytotoxic chemotherapy until progression vs observation in terms of PFS (hazard ratio, 0.71; 95% CI, 0.46-1.09) and OS (hazard ratio, 0.95; 95% CI, 0.85-1.07). Compared with observation, maintenance therapy showed a PFS benefit (hazard ratio, 0.58; 95% CI, 0.43-0.77) but not an OS benefit (hazard ratio, 0.91; 95% CI, 0.83-1.01). All maintenance strategies (FP, FP + Bev, and Bev) showed significant improvement in PFS vs observation. On SUCRA analysis, maintenance treatment (FP or FP + Bev) had the highest likelihood of achieving improved PFS (67.1% for FP, 99.8% for FP + Bev, and 36.5% for Bev) and OS (81.3% for FP, 73.2% for FP + Bev, and 32.6% for Bev).
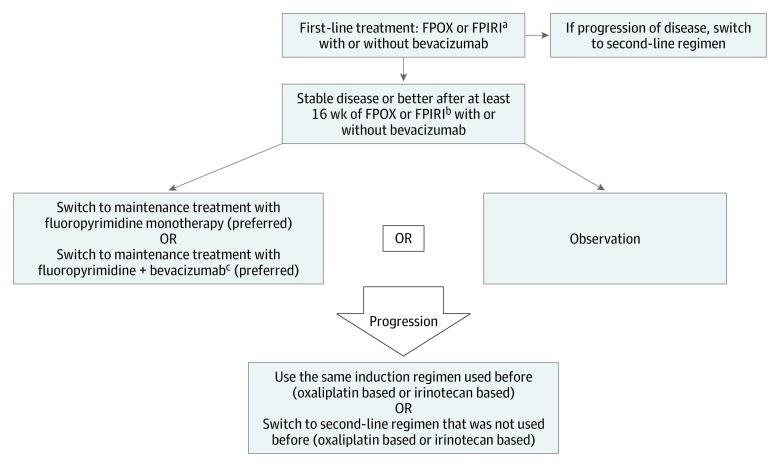
Conclusions and relevance: For patients with metastatic colorectal cancer, there is no benefit to continuing the full induction regimen until progression, without a period of either observation or maintenance treatment. A maintenance strategy with a fluoropyrimidine, with or without the addition of bevacizumab, is preferred. However, given the lack of a clear OS benefit, shared decision-making should include observation as an acceptable alternative.
Conflict of interest statement
Figures
Comment in
-
The Role of Maintenance Therapy in Metastatic Colorectal Cancer.JAMA Oncol. 2020 Jun 1;6(6):937. doi: 10.1001/jamaoncol.2020.0580. JAMA Oncol. 2020. PMID: 32297912 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
