

Ischemic and Bleeding Outcomes in Patients With Atrial Fibrillation and Contraindications to Oral Anticoagulation
- PMID: 31857036
- PMCID: PMC6927541
- DOI: 10.1016/j.jacep.2019.07.011
Ischemic and Bleeding Outcomes in Patients With Atrial Fibrillation and Contraindications to Oral Anticoagulation
Abstract
Objectives: This study sought to describe clinical outcomes among patients with atrial fibrillation (AF) and contraindications to oral anticoagulation (OAC).
Background: Treatment with OAC prevents stroke and death in patients with AF, but may be contraindicated among patients at high bleeding risk.
Methods: This was an observational, longitudinal analysis of a nationally representative 5% Medicare sample of patients with chronic AF and CHA2DS2-VASc (congestive heart failure, hypertension, age ≥75 years, diabetes mellitus, prior stroke or transient ischemic attack or thromboembolism, vascular disease, age 65-74 years, sex category) score ≥2. They were stratified by both the presence of high bleeding risk contraindications to OAC and by OAC use. We assessed 3-year ischemic and bleeding outcomes using multivariable Cox proportional hazards models adjusted for relevant patient characteristics.
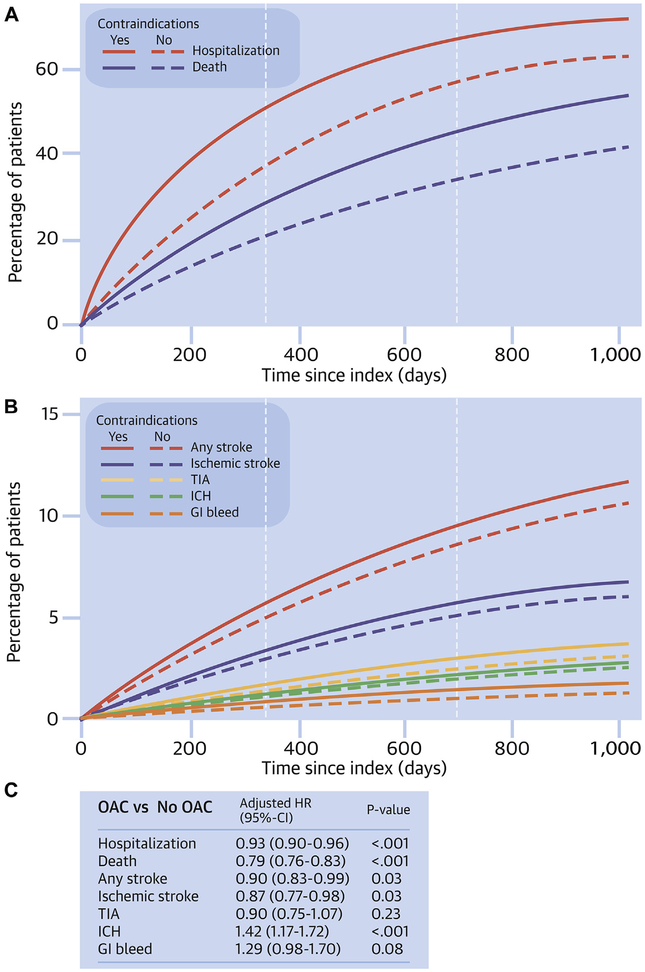
Results: Among 26,684 AF patients not treated with OAC, 8,283 (31%) had a high bleeding risk contraindication, primarily a blood dyscrasia (75%) or history of gastrointestinal bleeding (40%). Without OAC, patients with contraindications had worse ischemic and bleeding outcomes at 3 years compared with those without contraindications. We also identified 12,454 patients with OAC contraindications who received OAC. Compared with patients not receiving OAC, use of OAC was associated with reduced mortality (adjusted hazard ratio [HR]: 0.79; 95% confidence interval [CI]: 0.76 to 0.83), stroke (adjusted HR: 0.90; 95% CI: 0.83 to 0.99), and all-cause hospitalization (adjusted HR: 0.93; 95% CI: 0.90 to 0.96) but increased risk of intracranial hemorrhage (adjusted HR: 1.42; 95% CI: 1.17 to 1.72).
Conclusions: High bleeding risk contraindications to OAC are common among older patients with AF, and these patients have higher mortality compared with untreated patients without OAC contraindications. The use of OAC in these patients is associated with lower rates of all-cause stroke, hospitalization, and death but higher risk of intracranial hemorrhage.
Keywords: Medicare; anticoagulation; atrial fibrillation; contraindication; outcomes.
Copyright © 2019 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Contraindication to Anticoagulation in Nonvalvular Atrial Fibrillation: Are We Still to Fear the Clot and Not the Bleed?JACC Clin Electrophysiol. 2019 Dec;5(12):1393-1395. doi: 10.1016/j.jacep.2019.07.008. Epub 2019 Sep 26. JACC Clin Electrophysiol. 2019. PMID: 31857037 No abstract available.
References
-
- Hart RG, Benavente O, McBride R, Pearce LA. Antithrombotic therapy to prevent stroke in patients with atrial fibrillation: a meta-analysis. Ann Intern Med 1999;131:492–501. - PubMed
-
- Camm AJ, Lip GY, De Caterina R, et al. 2012 focused update of the ESC Guidelines for the management of atrial fibrillation: an update of the 2010 ESC Guidelines for the management of atrial fibrillation. Developed with the special contribution of the European Heart Rhythm Association. Eur Heart J 2012; 33:2719–47. - PubMed
-
- Wann LS, Curtis AB, January CT, et al. 2011 ACCF/AHA/HRS focused update on the management of patients with atrial fibrillation (updating the 2006 guideline): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2011;57: 1330–7. - PubMed
-
- Fang MC, Stafford RS, Ruskin JN, Singer DE. National trends in antiarrhythmic and antithrombotic medication use in atrial fibrillation. Arch Intern Med 2004;164:55–60. - PubMed
-
- Gage BF, Boechler M, Doggette AL, et al. Adverse outcomes and predictors of underuse of antithrombotic therapy in medicare beneficiaries with chronic atrial fibrillation. Stroke 2000;31: 822–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
