

2019 Update to: Management of Hyperglycemia in Type 2 Diabetes, 2018. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD)
- PMID: 31857443
- PMCID: PMC6971782
- DOI: 10.2337/dci19-0066
2019 Update to: Management of Hyperglycemia in Type 2 Diabetes, 2018. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD)
Erratum in
-
Erratum. 2019 Update to: Management of Hyperglycemia in Type 2 Diabetes, 2018. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2020;43:487-493.Diabetes Care. 2020 Jul;43(7):1670. doi: 10.2337/dc20-er07. Epub 2020 May 22. Diabetes Care. 2020. PMID: 32444453 Free PMC article. No abstract available.
Abstract
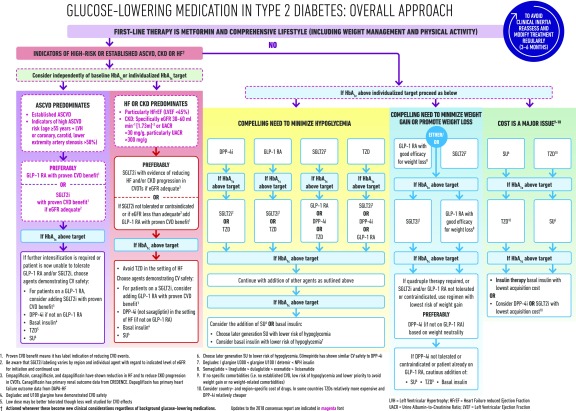
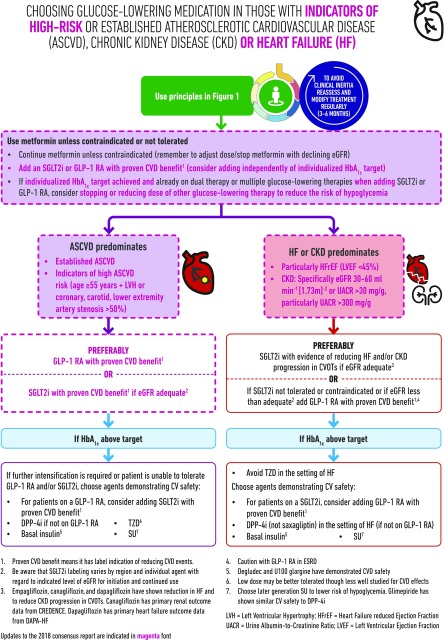
The American Diabetes Association and the European Association for the Study of Diabetes have briefly updated their 2018 recommendations on management of hyperglycemia, based on important research findings from large cardiovascular outcomes trials published in 2019. Important changes include: 1) the decision to treat high-risk individuals with a glucagon-like peptide 1 (GLP-1) receptor agonist or sodium-glucose cotransporter 2 (SGLT2) inhibitor to reduce major adverse cardiovascular events (MACE), hospitalization for heart failure (hHF), cardiovascular death, or chronic kidney disease (CKD) progression should be considered independently of baseline HbA1c or individualized HbA1c target; 2) GLP-1 receptor agonists can also be considered in patients with type 2 diabetes without established cardiovascular disease (CVD) but with the presence of specific indicators of high risk; and 3) SGLT2 inhibitors are recommended in patients with type 2 diabetes and heart failure, particularly those with heart failure with reduced ejection fraction, to reduce hHF, MACE, and CVD death, as well as in patients with type 2 diabetes with CKD (estimated glomerular filtration rate 30 to ≤60 mL min-1 [1.73 m]-2 or urinary albumin-to-creatinine ratio >30 mg/g, particularly >300 mg/g) to prevent the progression of CKD, hHF, MACE, and cardiovascular death.
© 2019 by the American Diabetes Association.
Figures
References
-
- Davies MJ, D’Alessio DA, Fradkin J, et al. . Management of hyperglycaemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia 2018;61:2461–2498 - PubMed
-
- Gerstein HC, Colhoun HM, Dagenais GR, et al. .; REWIND Investigators . Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): a double-blind, randomised placebo-controlled trial. Lancet 2019;394:121–130 - PubMed
-
- Wiviott SD, Raz I, Bonaca MP, et al. .; DECLARE–TIMI 58 Investigators . Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2019;380:347–357 - PubMed
-
- Zelniker TA, Wiviott SD, Raz I, et al. . Comparison of the effects of glucagon-like peptide receptor agonists and sodium-glucose cotransporter 2 inhibitors for prevention of major adverse cardiovascular and renal outcomes in type 2 diabetes mellitus. Circulation 2019;139:2022–2031 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
