

The burden of comorbidities in pulmonary arterial hypertension
- PMID: 31857797
- PMCID: PMC6915052
- DOI: 10.1093/eurheartj/suz205
The burden of comorbidities in pulmonary arterial hypertension
Abstract
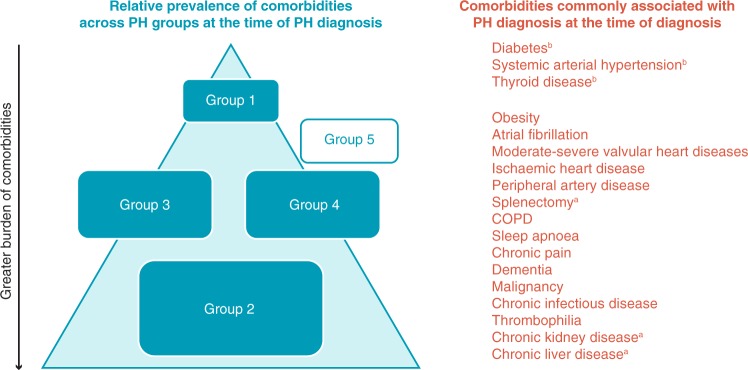
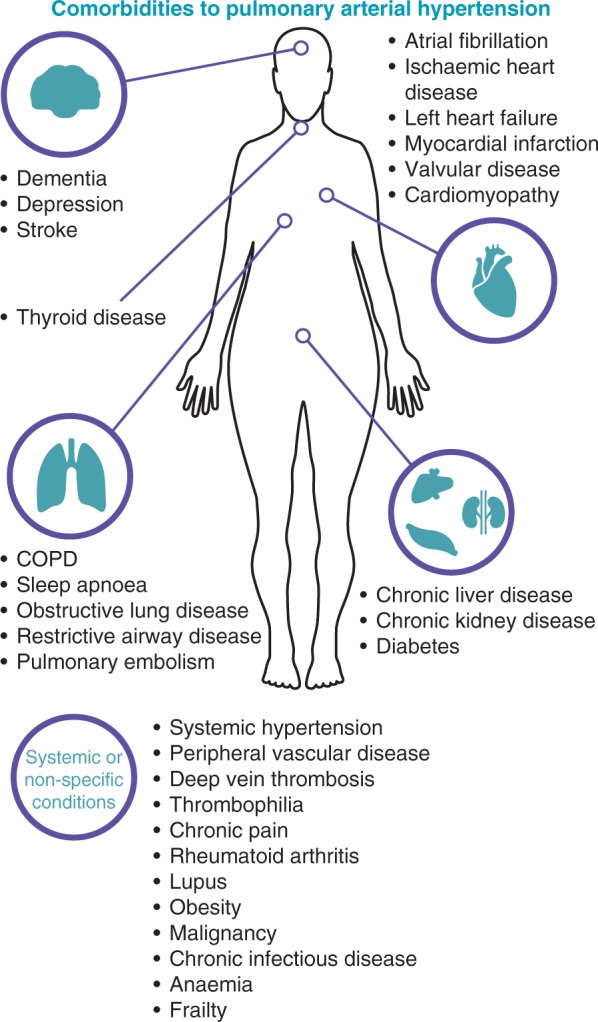
Patients with comorbidities are often excluded from clinical trials, limiting the evidence base for pulmonary arterial hypertension (PAH)-specific therapies. This review aims to discuss the effect of comorbidities on the diagnosis and management of PAH. The comorbidities discussed in this review (systemic hypertension, obesity, sleep apnoea, clinical depression, obstructive airway disease, thyroid disease, diabetes, and ischaemic cardiovascular event) were chosen based on their prevalence in patients with idiopathic PAH in the REVEAL registry (Registry to EValuate Early and Long-term PAH disease management). Comorbidities can mask the symptoms of PAH, leading to delays in diagnosis and also difficulty evaluating disease progression and treatment effects. Due to the multifactorial pathophysiology of pulmonary hypertension (PH), the presence of comorbidities can lead to difficulties in distinguishing between Group 1 PH (PAH) and the other group classifications of PH. Many comorbidities contribute to the progression of PAH through increased pulmonary artery pressures and cardiac output, therefore treatment of the comorbidity may also reduce the severity of PAH. Similarly, the development of one comorbidity can be a risk factor for the development of other comorbidities. The management of comorbidities requires consideration of drug interactions, polypharmacy, adherence and evidence-based strategies. A multidisciplinary team should be involved in the management of patients with PAH and comorbidities, with appropriate referral to supportive services when necessary. The treatment goals and expectations of patients must be managed in the context of comorbidities.
Keywords: Comorbidities; Diagnosis; Management; Pulmonary arterial hypertension; Treatment.
Published on behalf of the European Society of Cardiology. © The Author(s) 2019.
Figures
References
-
- Feinstein AR. The pre-therapeutic classification of co-morbidity in chronic disease. J Chronic Dis 1970;23:455–468. - PubMed
-
- Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B.. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet 2012;380:37–43. - PubMed
-
- Hjalmarsson C, Radegran G, Kylhammar D, Rundqvist B, Multing J, Nisell MD, Kjellstrom B.. Impact of age and comorbidity on risk stratification in idiopathic pulmonary arterial hypertension. Eur Respir J 2018;51:1702310.. - PubMed
-
- Ling Y, Johnson MK, Kiely DG, Condliffe R, Elliot CA, Gibbs JS, Howard LS, Pepke-Zaba J, Sheares KK, Corris PA, Fisher AJ, Lordan JL, Gaine S, Coghlan JG, Wort SJ, Gatzoulis MA, Peacock AJ.. Changing demographics, epidemiology, and survival of incident pulmonary arterial hypertension: results from the pulmonary hypertension registry of the United Kingdom and Ireland. Am J Respir Crit Care Med 2012;186:790–796. - PubMed