

Oral Leukoplakia and Risk of Progression to Oral Cancer: A Population-Based Cohort Study
- PMID: 31860085
- PMCID: PMC7566351
- DOI: 10.1093/jnci/djz238
Oral Leukoplakia and Risk of Progression to Oral Cancer: A Population-Based Cohort Study
Abstract
Background: The optimal clinical management of oral precancer remains uncertain. We investigated the natural history of oral leukoplakia, the most common oral precancerous lesion, to estimate the relative and absolute risks of progression to cancer, the predictive accuracy of a clinician's decision to biopsy a leukoplakia vis-à-vis progression, and histopathologic predictors of progression.
Methods: We conducted a retrospective cohort study (1996-2012) of patients with oral leukoplakia (n = 4886), identified using electronic medical records within Kaiser Permanente Northern California. Among patients with leukoplakia who received a biopsy (n = 1888), we conducted a case-cohort study to investigate histopathologic predictors of progression. Analyses included indirect standardization and unweighted or weighted Cox regression.
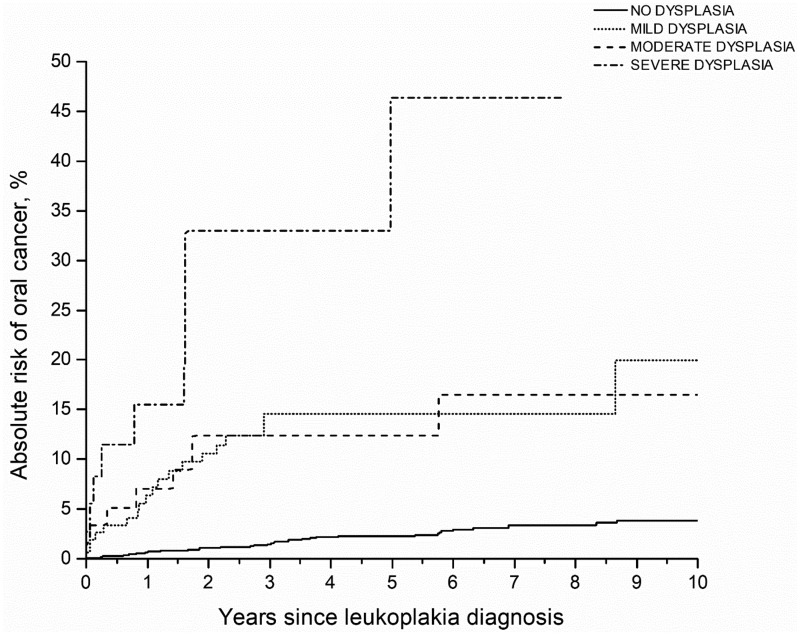
Results: Compared with the overall Kaiser Permanente Northern California population, oral cancer incidence was substantially elevated in oral leukoplakia patients (standardized incidence ratio = 40.8, 95% confidence interval [CI] = 34.8 to 47.6; n = 161 cancers over 22 582 person-years). Biopsied leukoplakias had a higher oral cancer risk compared with those that were not biopsied (adjusted hazard ratio = 2.38, 95% CI = 1.73 to 3.28). However, to identify a prevalent or incident oral cancer, the biopsy decision had low sensitivity (59.6%), low specificity (62.1%), and moderate positive-predictive value (5.1%). Risk of progression to oral cancer statistically significantly increased with the grade of dysplasia; 5-year competing risk-adjusted absolute risks were: leukoplakia overall = 3.3%, 95% CI = 2.7% to 3.9%; no dysplasia = 2.2%, 95% CI = 1.5% to 3.1%; mild-dysplasia = 11.9%, 95% CI = 7.1% to 18.1%; moderate-dysplasia = 8.7%, 95% CI = 3.2% to 17.9%; and severe dysplasia = 32.2%, 95% CI = 8.1%-60.0%. Yet 39.6% of cancers arose from biopsied leukoplakias without dysplasia.
Conclusions: The modest accuracy of the decision to biopsy a leukoplakia vis-à-vis presence or eventual development of oral cancer highlights the need for routine biopsy of all leukoplakias regardless of visual or clinical impression. Leukoplakia patients, particularly those with dysplasia, need to be closely monitored for signs of early cancer.
Published by Oxford University Press 2019. This work is written by US Government employees and is in the public domain in the US.
Figures
Comment in
-
Response to Brandt, Bednarz-Knoll, Kleinheinz et al.J Natl Cancer Inst. 2020 Sep 1;112(9):970-971. doi: 10.1093/jnci/djaa075. J Natl Cancer Inst. 2020. PMID: 32483585 Free PMC article. No abstract available.
-
RE: Oral Leukoplakia and Risk of Progression to Oral Cancer: A Population-Based Cohort Study.J Natl Cancer Inst. 2020 Sep 1;112(9):968-969. doi: 10.1093/jnci/djaa074. J Natl Cancer Inst. 2020. PMID: 32483602 Free PMC article. No abstract available.
References
-
- Shield KD, Ferlay J, Jemal A, Sankaranarayanan R, Chaturvedi AK, Bray F, et al. The global incidence of lip, oral cavity, and pharyngeal cancers by subsite in 2012. CA Cancer J Clin. 2017;67(1):51–64. - PubMed
-
- Napier SS, Speight PM.. Natural history of potentially malignant oral lesions and conditions: an overview of the literature. J Oral Pathol Med. 2008;37(1):1–10. - PubMed
-
- Chi AC, Day TA, Neville BW.. Oral cavity and oropharyngeal squamous cell carcinoma—an update. CA Cancer J Clin. 2015;65(5):401–421. - PubMed
-
- Neville BW, Day TA.. Oral cancer and precancerous lesions. CA Cancer J Clin. 2002;52(4):195–215. - PubMed
-
- Moyer VA, Force U.. Screening for oral cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2014;160(1):55–60. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
