Trypanosoma cruzi infection in puerperal women and their neonates at Barcelona, Anzoategui State, Venezuela
- PMID: 31860187
- PMCID: PMC7363338
- DOI: 10.7705/biomedica.4606
Trypanosoma cruzi infection in puerperal women and their neonates at Barcelona, Anzoategui State, Venezuela
Abstract
Introduction. Trypanosoma cruzi is mainly transmitted by vectors. Other pathways such as oral and congenital transmission have become increasingly relevant. Objective. To evaluate T. cruzi infections in post-partum women and their newborns who attended the Hospital Universitario Dr. Luis Razetti (Barcelona, Anzoátegui state, Venezuela). Materials and methods. A prospective cross-sectional study was undertaken from May, 2015, to August, 2016. ELISA, MABA and IFI assays were used to determine the infection in 1,200 post-partum women. The newborns of seropositive women were then examined for T. cruzi by PCR amplification and serological tests at nine months old. The prevalence of the parasitic infection in post-partum women and their newborns was then estimated. To establish the relationship between risk factors and infection, the chi-square test (c2) and the probability ratio (OR) was applied. Results. A total of 78 women were identified as seropositive (6.50 %) (CI 95%: 5.10-7.89%), and parasitic DNA was detected in six of their newborns (9.09%). Nine months after birth eleven infants were examined, and all were found to be serologically negative. Risk factors detected were pregnancy duration (OR: 0,36; CI95%: 0,15-0,84), where the patients lived at present (OR: 0,34; CI95%: 0,24-0,62) or previously (OR: 2,50; CI95%: 1,38-4,52) and having relatives with Chagas disease (OR: 1,75; CI95%: 1,02-3,01). Conclusions. Seroprevalence for T. cruzi infection in young post-partum women in rural areas was high. The detection of parasite DNA at birth was not indicative of congenital Chagas disease.
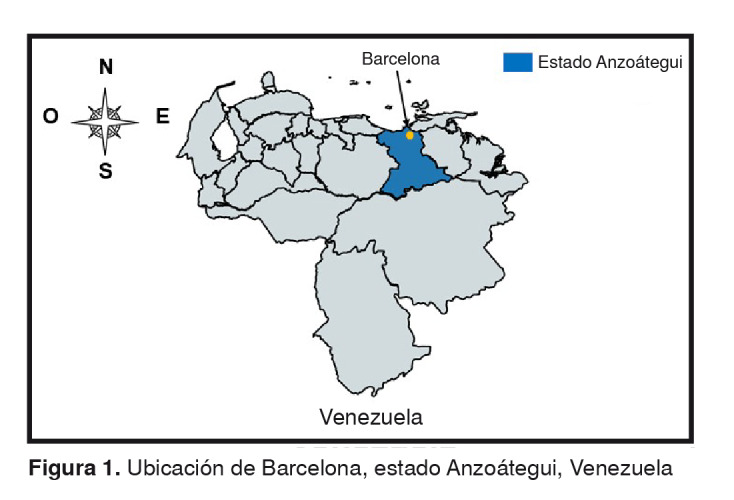
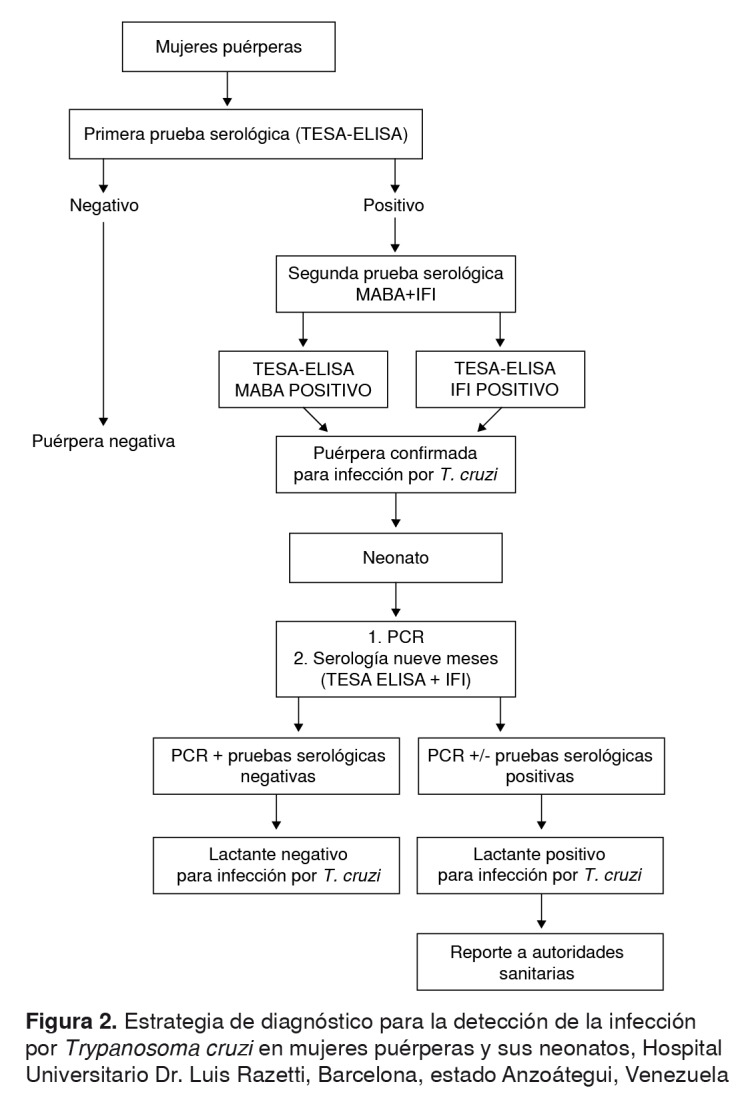
Introducción. Trypanosoma cruzi se transmite principalmente por vía vectorial, sin embargo, las rutas oral y congénita han tomado relevancia. Objetivo. Evaluar la infección por T. cruzi en mujeres puérperas y sus neonatos en el Hospital Universitario Dr. Luis Razetti de Barcelona, estado Anzoátegui, Venezuela. Materiales y métodos. Se hizo un estudio prospectivo de corte transversal, de mayo de 2015 a agosto de 2016, en el que se evaluaron 1.200 mujeres para determinar la infección mediante las pruebas ELISA, MABA e IFI. Los neonatos de las madres seropositivas se evaluaron con la prueba de PCR y por serología a los nueve meses de edad. Se estimó la prevalencia de la infección por T. cruzi en mujeres puérperas y sus neonatos. Para establecer los factores de riesgo asociados a la infección, se usó la prueba de ji al cuadrado (c2) y la razón de probabilidad (OR). Resultados. En total, 78 (6,50 %) mujeres resultaron positivas (IC95% 5,10-7,89 %). En seis (9,09 %) recién nacidos de madres seropositivas, se detectó ADN parasitario. Tras nueve meses de nacidos, once lactantes evaluados resultaron serológicamente negativos. La infección estuvo asociada con la duración del embarazo (OR=0,36; IC95% 0,15-0,84), origen del domicilio actual (OR=0,34; IC95% 0,24-0,62) o previo (OR=2,50; IC95% 1,38-4,52) y el tener familiares con la enfermedad de Chagas (OR=1,75; IC95% 1,02-3,01). Conclusiones. La seroprevalencia para la infección por T. cruzi en mujeres puérperas del medio rural, fue elevada. La detección de ADN parasitario al momento del nacimiento no es indicativa de enfermedad de Chagas congénita.
Keywords: Trypanosoma cruzi; Chagas diseases/diagnosis; newborn; enzyme-linked immunosorbent assay; Venezuela.
Conflict of interest statement
Figures
Similar articles
-
Trypanosoma cruzi seroprevalence in pregnant women and screening by PCR and microhaematocrit in newborns from Guanajuato, Mexico.Acta Trop. 2016 Dec;164:100-106. doi: 10.1016/j.actatropica.2016.08.029. Epub 2016 Sep 3. Acta Trop. 2016. PMID: 27596439
-
Maternal fetal transmission of Trypanosoma cruzi: a problem of public health little studied in Mexico.Exp Parasitol. 2012 Aug;131(4):425-32. doi: 10.1016/j.exppara.2012.05.013. Epub 2012 Jun 7. Exp Parasitol. 2012. PMID: 22683499
-
Do commercial serologic tests for Trypanosoma cruzi infection detect Mexican strains in women and newborns?J Parasitol. 2011 Apr;97(2):338-43. doi: 10.1645/GE-2545.1. Epub 2010 Oct 21. J Parasitol. 2011. PMID: 21506787 Free PMC article.
-
Update on Chagas disease in Venezuela during the period 2003-2018. A review.Acta Trop. 2020 Mar;203:105310. doi: 10.1016/j.actatropica.2019.105310. Epub 2019 Dec 17. Acta Trop. 2020. PMID: 31862464 Review.
-
Congenital transmission of Chagas disease: a clinical approach.Expert Rev Anti Infect Ther. 2010 Aug;8(8):945-56. doi: 10.1586/eri.10.74. Expert Rev Anti Infect Ther. 2010. PMID: 20695749 Review.
Cited by
-
Ten years follow-up of the largest oral Chagas disease outbreak: Cardiological prospective cohort study.PLoS Negl Trop Dis. 2023 Oct 6;17(10):e0011643. doi: 10.1371/journal.pntd.0011643. eCollection 2023 Oct. PLoS Negl Trop Dis. 2023. PMID: 37801449 Free PMC article.
-
Predictor Variables in the Spread of Chagas Disease in Rural Areas.Pathogens. 2024 May 8;13(5):394. doi: 10.3390/pathogens13050394. Pathogens. 2024. PMID: 38787245 Free PMC article.
-
Prenatal Chagas disease screening in Latin America: the current policy landscape and potential utility of an expanded maternal-familial Trypanosoma cruzi testing framework.Lancet Reg Health Am. 2025 May 27;47:101139. doi: 10.1016/j.lana.2025.101139. eCollection 2025 Jul. Lancet Reg Health Am. 2025. PMID: 40502726 Free PMC article. Review.
References
-
- World Health Organization Chagas disease in Latin America: An epidemiological update based on 2010 estimates. Wkly Epidemiol Rec. 2015;90:33–43. - PubMed
-
- Colimon KM. Fundamentos de epidemiología. Tercera edición. Medellín: Coorporación para Investigaciones Biológicas; 2010. pp. 551–551.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous