

The Hospital Readmissions Reduction Program and Readmissions for Chronic Obstructive Pulmonary Disease, 2006-2015
- PMID: 31860333
- PMCID: PMC7175978
- DOI: 10.1513/AnnalsATS.201909-672OC
The Hospital Readmissions Reduction Program and Readmissions for Chronic Obstructive Pulmonary Disease, 2006-2015
Abstract
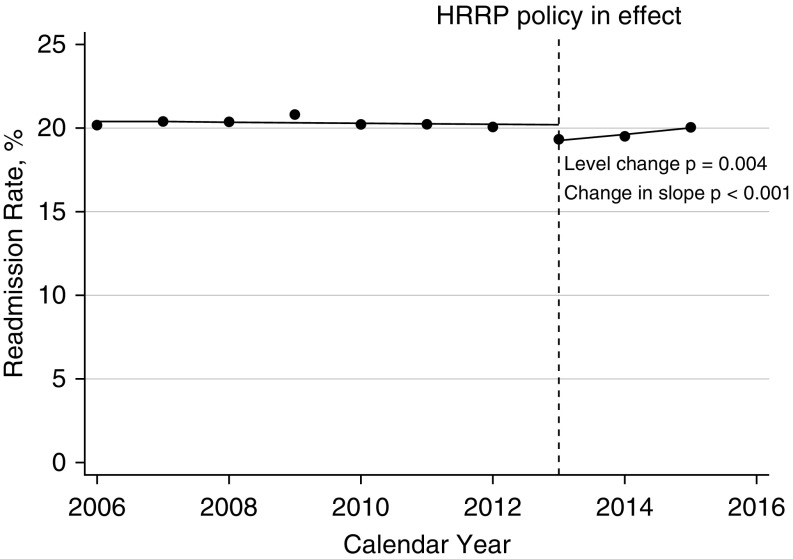
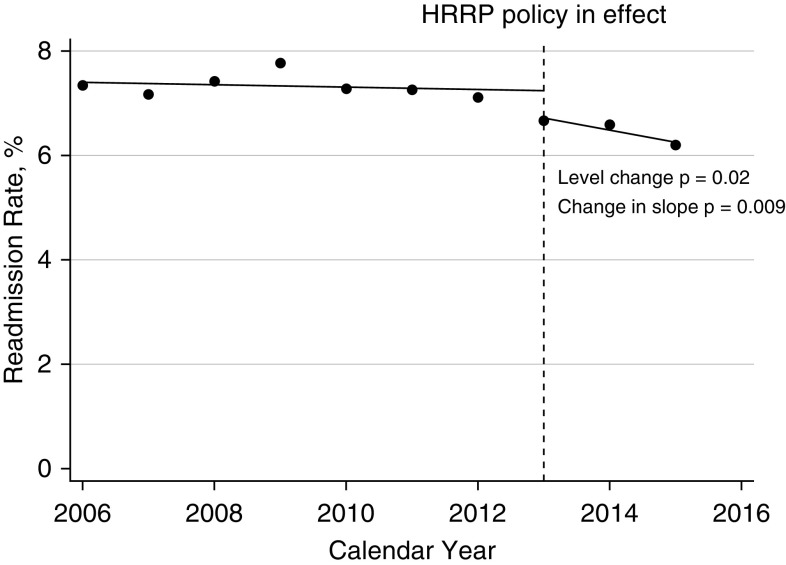
Rationale: In October 2012, the initial phase of the Hospital Readmission Reduction Program imposed financial penalties on hospitals with higher-than-expected risk-adjusted 30-day readmission rates for Medicare beneficiaries with congestive heart failure, myocardial infarction, and pneumonia. We hypothesized that these penalties may also be associated with decreased readmissions for chronic obstructive pulmonary disease (COPD) in the general population before COPD became a target condition (October 2014).Objectives: To determine if implementation of the initial financial penalties for other conditions was associated with a decrease in hospital readmissions for COPD.Methods: We used population-level data to examine patients readmitted for any reason or for COPD within 30 days after an initial hospitalization for COPD. The data source was seven states in the State Inpatient Database. The preimplementation period included calendar years 2006 to 2012. The postimplementation period included 2013 to 2015. Using interrupted time series, the level change was examined, which reflected the difference between the expected and actual readmission rates in 2013. The difference in slopes between the pre- and postimplementation periods was also examined.Results: We identified 805,764 hospitalizations for COPD from 904 hospitals. Overall, 26% of patients had primary insurance other than Medicare. After the intervention, patients had lower rates of all-cause 30-day readmissions (level change, -0.93%; 95% confidence interval [CI], -1.44% to -0.43%; P = 0.004), which was driven by fewer early readmissions (0-7 d). The postimplementation slope became positive; the difference in slopes was 0.39% (95% CI, 0.28% to 0.50%; P < 0.001). Patients also had lower rates of COPD-related readmissions (level decrease, -0.52%; 95% CI, -0.93% to -0.12%; P = 0.02), which was due to decreases in both early and late (8-30 d) readmissions. The postimplementation slope was negative; the difference in slopes was -0.21% (95% CI, -0.35% to -0.07%; P = 0.009).Conclusions: In patients with COPD and any insurance status, there was an association between the initial phase of the Hospital Readmission Reduction Program and a decrease in both all-cause and COPD-related readmissions even before COPD became a target diagnosis. The large amount of money at risk to hospitals likely resulted in broad behavioral change. Future research is needed to test which levers can effectively reduce readmission rates for COPD.
Keywords: COPD; health policy; hospital readmissions.
Figures
Comment in
-
Moving the Bar on Chronic Obstructive Pulmonary Disease Readmissions before and after the Hospital Readmission Reduction Program: Myth or Reality?Ann Am Thorac Soc. 2020 Apr;17(4):423-425. doi: 10.1513/AnnalsATS.202001-010ED. Ann Am Thorac Soc. 2020. PMID: 32233856 No abstract available.
References
-
- Perera PN, Armstrong EP, Sherrill DL, Skrepnek GH. Acute exacerbations of COPD in the United States: inpatient burden and predictors of costs and mortality. COPD. 2012;9:131–141. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
