

Comparative effects of 18 antipsychotics on metabolic function in patients with schizophrenia, predictors of metabolic dysregulation, and association with psychopathology: a systematic review and network meta-analysis
- PMID: 31860457
- PMCID: PMC7029416
- DOI: 10.1016/S2215-0366(19)30416-X
Comparative effects of 18 antipsychotics on metabolic function in patients with schizophrenia, predictors of metabolic dysregulation, and association with psychopathology: a systematic review and network meta-analysis
Abstract
Background: Antipsychotic treatment is associated with metabolic disturbance. However, the degree to which metabolic alterations occur in treatment with different antipsychotics is unclear. Predictors of metabolic dysregulation are poorly understood and the association between metabolic change and change in psychopathology is uncertain. We aimed to compare and rank antipsychotics on the basis of their metabolic side-effects, identify physiological and demographic predictors of antipsychotic-induced metabolic dysregulation, and investigate the relationship between change in psychotic symptoms and change in metabolic parameters with antipsychotic treatment.
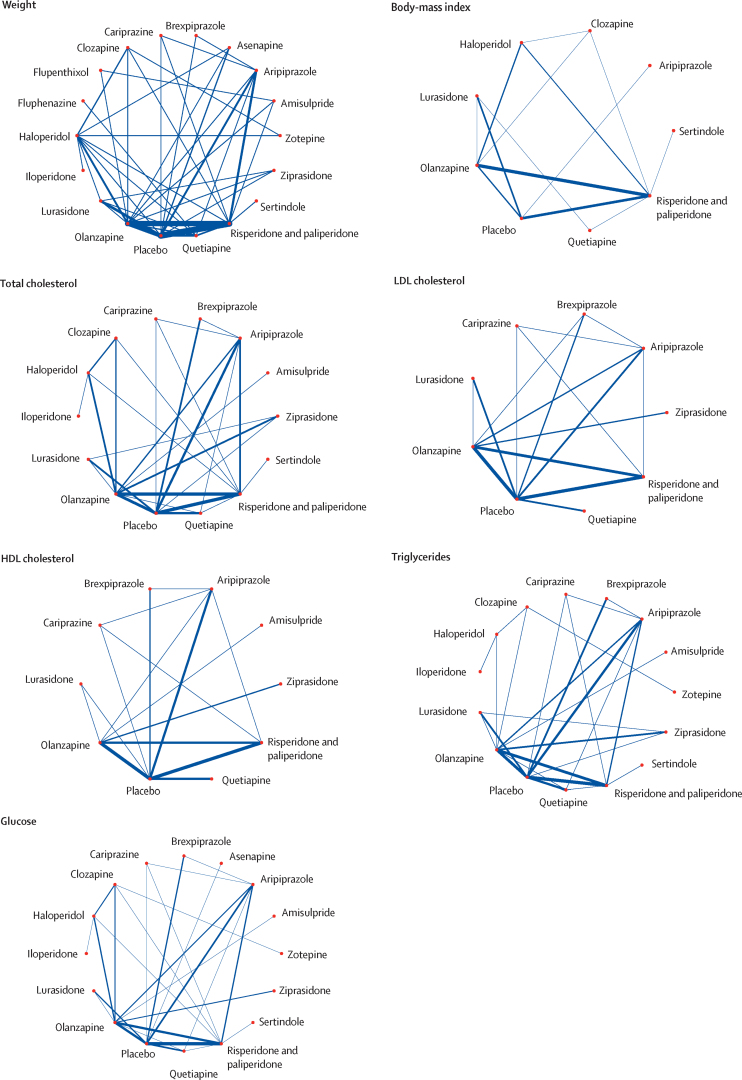
Methods: We searched MEDLINE, EMBASE, and PsycINFO from inception until June 30, 2019. We included blinded, randomised controlled trials comparing 18 antipsychotics and placebo in acute treatment of schizophrenia. We did frequentist random-effects network meta-analyses to investigate treatment-induced changes in body weight, BMI, total cholesterol, LDL cholesterol, HDL cholesterol, triglyceride, and glucose concentrations. We did meta-regressions to examine relationships between metabolic change and age, sex, ethnicity, baseline weight, and baseline metabolic parameter level. We examined the association between metabolic change and psychopathology change by estimating the correlation between symptom severity change and metabolic parameter change.
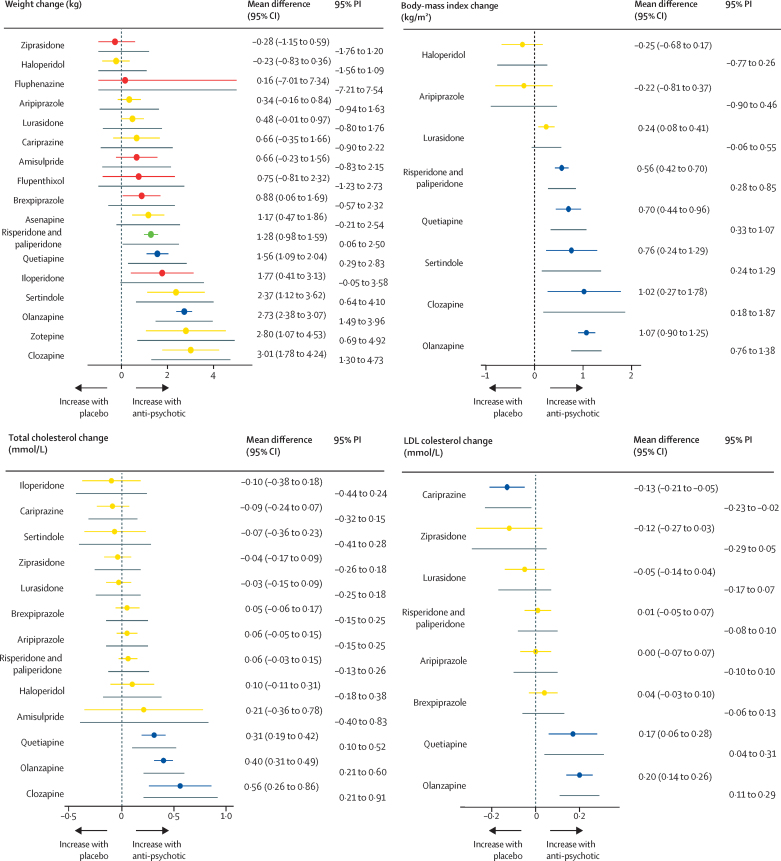
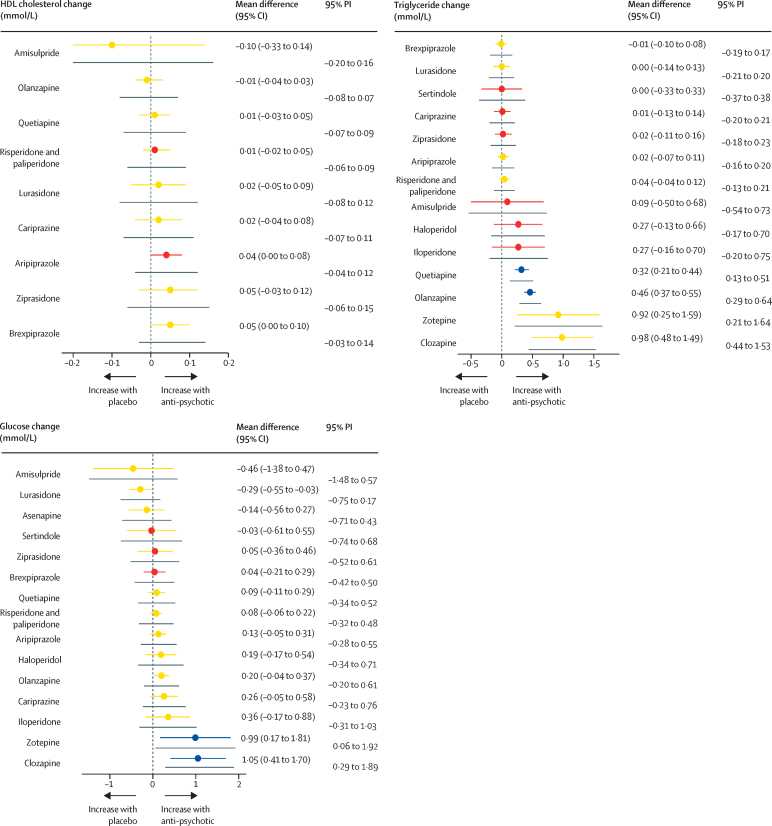
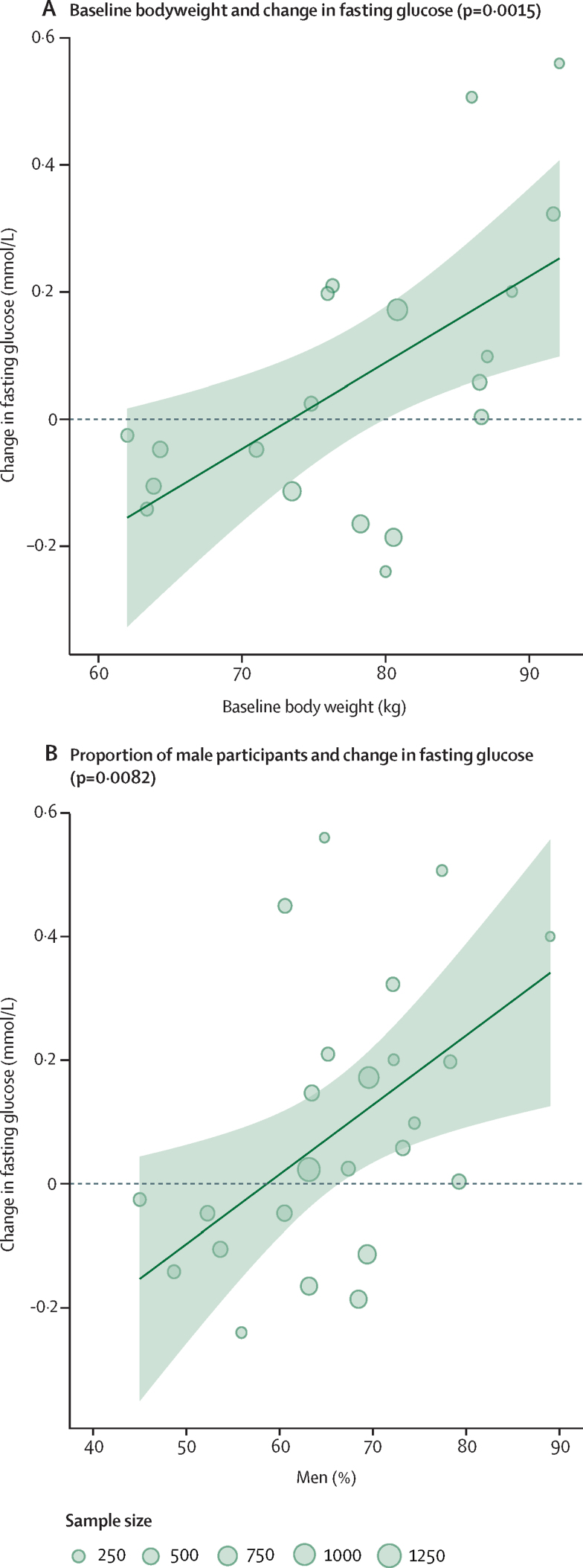
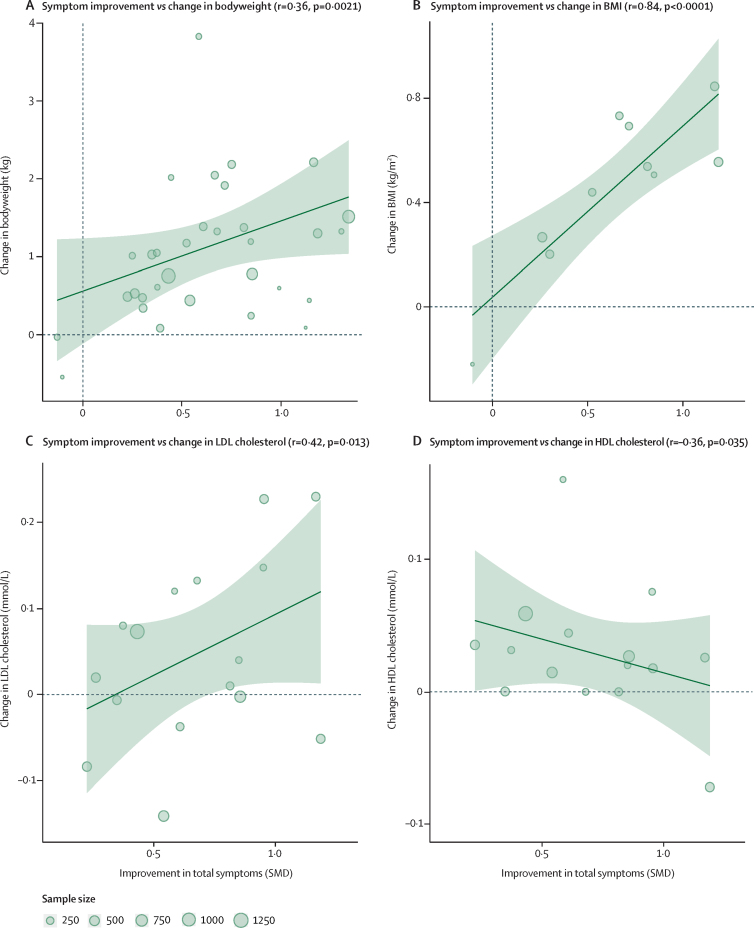
Findings: Of 6532 citations, we included 100 randomised controlled trials, including 25 952 patients. Median treatment duration was 6 weeks (IQR 6-8). Mean differences for weight gain compared with placebo ranged from -0·23 kg (95% CI -0·83 to 0·36) for haloperidol to 3·01 kg (1·78 to 4·24) for clozapine; for BMI from -0·25 kg/m2 (-0·68 to 0·17) for haloperidol to 1·07 kg/m2 (0·90 to 1·25) for olanzapine; for total-cholesterol from -0·09 mmol/L (-0·24 to 0·07) for cariprazine to 0·56 mmol/L (0·26-0·86) for clozapine; for LDL cholesterol from -0·13 mmol/L (-0.21 to -0·05) for cariprazine to 0·20 mmol/L (0·14 to 0·26) for olanzapine; for HDL cholesterol from 0·05 mmol/L (0·00 to 0·10) for brexpiprazole to -0·10 mmol/L (-0·33 to 0·14) for amisulpride; for triglycerides from -0·01 mmol/L (-0·10 to 0·08) for brexpiprazole to 0·98 mmol/L (0·48 to 1·49) for clozapine; for glucose from -0·29 mmol/L (-0·55 to -0·03) for lurasidone to 1·05 mmol/L (0·41 to 1·70) for clozapine. Greater increases in glucose were predicted by higher baseline weight (p=0·0015) and male sex (p=0·0082). Non-white ethnicity was associated with greater increases in total cholesterol (p=0·040) compared with white ethnicity. Improvements in symptom severity were associated with increases in weight (r=0·36, p=0·0021), BMI (r=0·84, p<0·0001), total-cholesterol (r=0·31, p=0·047), and LDL cholesterol (r=0·42, p=0·013), and decreases in HDL cholesterol (r=-0·35, p=0·035).
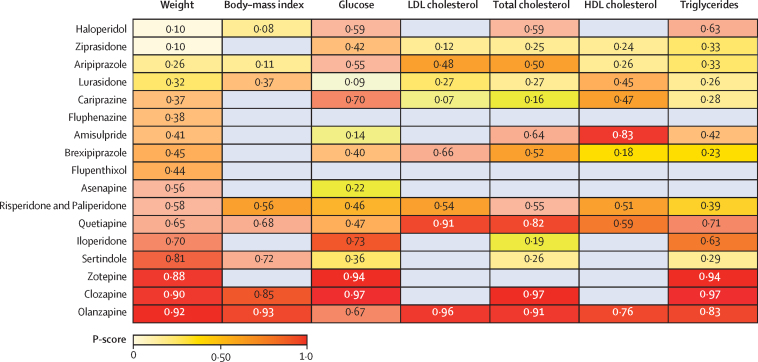
Interpretation: Marked differences exist between antipsychotics in terms of metabolic side-effects, with olanzapine and clozapine exhibiting the worst profiles and aripiprazole, brexpiprazole, cariprazine, lurasidone, and ziprasidone the most benign profiles. Increased baseline weight, male sex, and non-white ethnicity are predictors of susceptibility to antipsychotic-induced metabolic change, and improvements in psychopathology are associated with metabolic disturbance. Treatment guidelines should be updated to reflect our findings. However, the choice of antipsychotic should be made on an individual basis, considering the clinical circumstances and preferences of patients, carers, and clinicians.
Funding: UK Medical Research Council, Wellcome Trust, National Institute for Health Research Oxford Health Biomedical Research Centre.
Copyright © 2020 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Insights into metabolic dysregulations associated with antipsychotics.Lancet Psychiatry. 2020 Jan;7(1):6-7. doi: 10.1016/S2215-0366(19)30473-0. Epub 2019 Dec 17. Lancet Psychiatry. 2020. PMID: 31860456 No abstract available.
References
-
- Saha S, Chant D, McGrath J. A systematic review of mortality in schizophrenia: is the differential mortality gap worsening over time? Arch Gen Psychiatry. 2007;64:1123–1131. - PubMed
