

Polygenic risk-tailored screening for prostate cancer: A benefit-harm and cost-effectiveness modelling study
- PMID: 31860675
- PMCID: PMC6924639
- DOI: 10.1371/journal.pmed.1002998
Polygenic risk-tailored screening for prostate cancer: A benefit-harm and cost-effectiveness modelling study
Abstract
Background: The United States Preventive Services Task Force supports individualised decision-making for prostate-specific antigen (PSA)-based screening in men aged 55-69. Knowing how the potential benefits and harms of screening vary by an individual's risk of developing prostate cancer could inform decision-making about screening at both an individual and population level. This modelling study examined the benefit-harm tradeoffs and the cost-effectiveness of a risk-tailored screening programme compared to age-based and no screening.
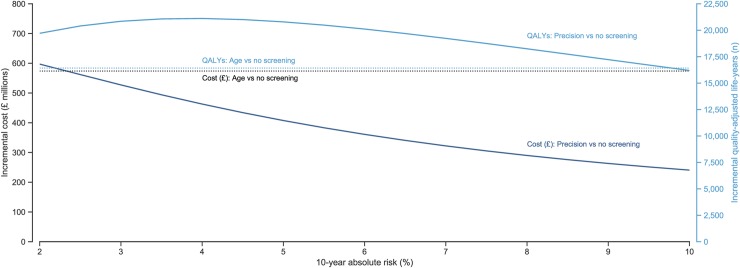
Methods and findings: A life-table model, projecting age-specific prostate cancer incidence and mortality, was developed of a hypothetical cohort of 4.48 million men in England aged 55 to 69 years with follow-up to age 90. Risk thresholds were based on age and polygenic profile. We compared no screening, age-based screening (quadrennial PSA testing from 55 to 69), and risk-tailored screening (men aged 55 to 69 years with a 10-year absolute risk greater than a threshold receive quadrennial PSA testing from the age they reach the risk threshold). The analysis was undertaken from the health service perspective, including direct costs borne by the health system for risk assessment, screening, diagnosis, and treatment. We used probabilistic sensitivity analyses to account for parameter uncertainty and discounted future costs and benefits at 3.5% per year. Our analysis should be considered cautiously in light of limitations related to our model's cohort-based structure and the uncertainty of input parameters in mathematical models. Compared to no screening over 35 years follow-up, age-based screening prevented the most deaths from prostate cancer (39,272, 95% uncertainty interval [UI]: 16,792-59,685) at the expense of 94,831 (95% UI: 84,827-105,630) overdiagnosed cancers. Age-based screening was the least cost-effective strategy studied. The greatest number of quality-adjusted life-years (QALYs) was generated by risk-based screening at a 10-year absolute risk threshold of 4%. At this threshold, risk-based screening led to one-third fewer overdiagnosed cancers (64,384, 95% UI: 57,382-72,050) but averted 6.3% fewer (9,695, 95% UI: 2,853-15,851) deaths from prostate cancer by comparison with age-based screening. Relative to no screening, risk-based screening at a 4% 10-year absolute risk threshold was cost-effective in 48.4% and 57.4% of the simulations at willingness-to-pay thresholds of GBP£20,000 (US$26,000) and £30,000 ($39,386) per QALY, respectively. The cost-effectiveness of risk-tailored screening improved as the threshold rose.
Conclusions: Based on the results of this modelling study, offering screening to men at higher risk could potentially reduce overdiagnosis and improve the benefit-harm tradeoff and the cost-effectiveness of a prostate cancer screening program. The optimal threshold will depend on societal judgements of the appropriate balance of benefits-harms and cost-effectiveness.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- UK National Screening Committee. The UK NSC recommendation on Prostate cancer screening/PSA testing in men over the age of 50 [Internet]. [cited 2018 Jul 13]. Available from: https://legacyscreening.phe.org.uk/prostatecancer
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
