

Concurrent treatment with rituximab and plasma exchange for severe refractory granulomatosis with polyangiitis: A case report
- PMID: 31860960
- PMCID: PMC6940185
- DOI: 10.1097/MD.0000000000018139
Concurrent treatment with rituximab and plasma exchange for severe refractory granulomatosis with polyangiitis: A case report
Abstract
Rationale: Rituximab is recommended to induce remission of severe granulomatosis with polyangiitis (GPA). Plasma exchange (PE) may be considered in the setting of rapidly progressive glomerulonephritis (RPGN) with a serum creatinine increase of more than 5.6 mg/dl or diffuse alveolar hemorrhage (DAH). However, there are no sufficient studies on combination therapy with rituximab and PE in GPA.
Patient concerns: A 23-year-old woman was admitted with fever, abdominal pain, and diarrhea on suspicion of infectious colitis. Colonoscopy showed hemorrhagic colitis and antibiotic treatment was ineffective. Physical examination revealed episcleritis and skin lesions similar to Janeway lesions or Osler nodes on her palms and soles. Transesophageal echocardiogram (TEE) revealed mitral valve vegetation mimicking infective endocarditis. However, no pathogen was grown in the blood culture. Ten days after admission, blood-tinged sputum and respiratory distress developed. Imaging studies of lung, bronchoscopy, and bronchoalveolar lavage indicated DAH. Moreover, serum creatinine levels rapidly increased from 0.8 mg/dl to 6.1 mg/dl with proteinuria.
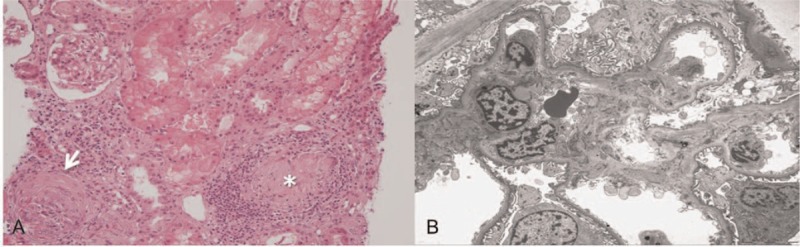
Diagnosis: The patient was diagnosed with GPA and non-infectious endocarditis, DAH, and RPGN, based on a biopsy which revealed pauci-immune crescentic glomerulonephritis with granuloma and leukocytoclastic vasculitis and antineutrophil cytoplasmic antibodies against proteinase 3- positivity.
Interventions: Initial methylprednisolone pulse therapy (1 g daily for 3 days) proved unsuccessful. After initiating PE, creatinine levels began to slowly decline, but DAH continued to deteriorate. Rituximab combined with PE therapy was considered. We performed PE every 2 to 3 days for 5 total treatments combined with rituximab (375 mg/m, once weekly for 4 weeks).
Outcomes: After the combination treatment of rituximab and PE, alveolar hemorrhage stopped. Chest X-ray and laboratory data, including serum creatinine and hemoglobin, notably improved. Mitral valve vegetation was no longer observed in follow-up TEE. GPA remained stable with low dose prednisolone and immunosuppressants over a follow-up period of 5 years.
Lessons: This case suggests that the use of rituximab and concurrent PE may represent a promising combination for severe and refractory GPA.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures



References
-
- Jones RB, Tervaert JW, Hauser T, et al. Rituximab versus cyclophosphamide in ANCA-associated renal vasculitis. N Engl J Med 2010;363:211–20. - PubMed
-
- Klemmer PJ, Chalermskulrat W, Reif MS, et al. Plasmapheresis therapy for diffuse alveolar hemorrhage in patients with small-vessel vasculitis. Am J Kidney Dis 2003;42:1149–53. - PubMed
-
- Jayne DR, Gaskin G, Rasmussen N, et al. Randomized trial of plasma exchange or high-dosage methylprednisolone as adjunctive therapy for severe renal vasculitis. J Am Soc Nephrol 2007;18:2180–8. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
