

Bionic Upper Limb Reconstruction: A Valuable Alternative in Global Brachial Plexus Avulsion Injuries-A Case Series
- PMID: 31861941
- PMCID: PMC7019829
- DOI: 10.3390/jcm9010023
Bionic Upper Limb Reconstruction: A Valuable Alternative in Global Brachial Plexus Avulsion Injuries-A Case Series
Abstract
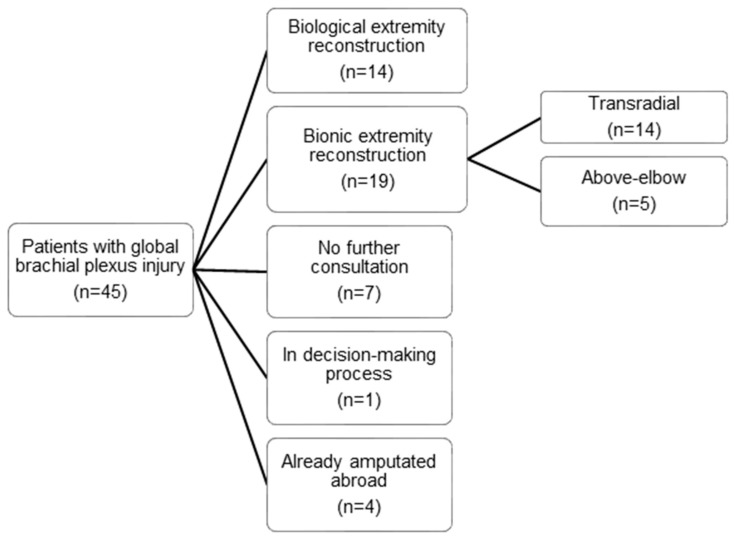
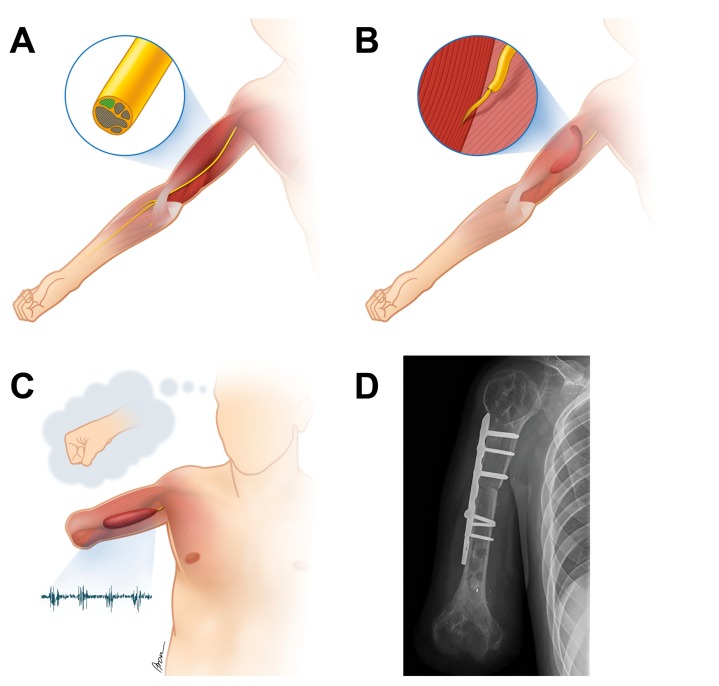
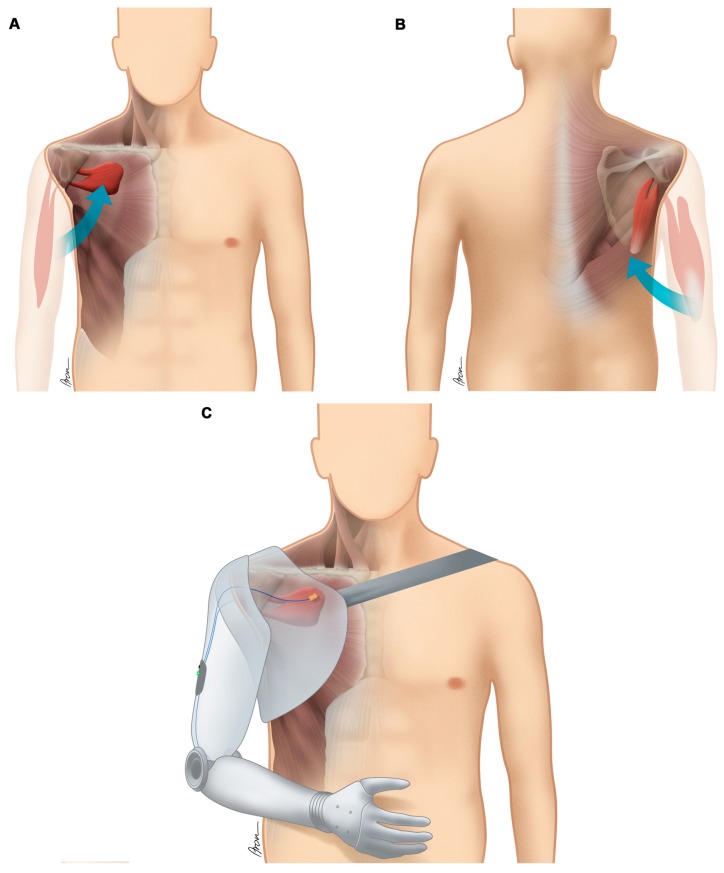
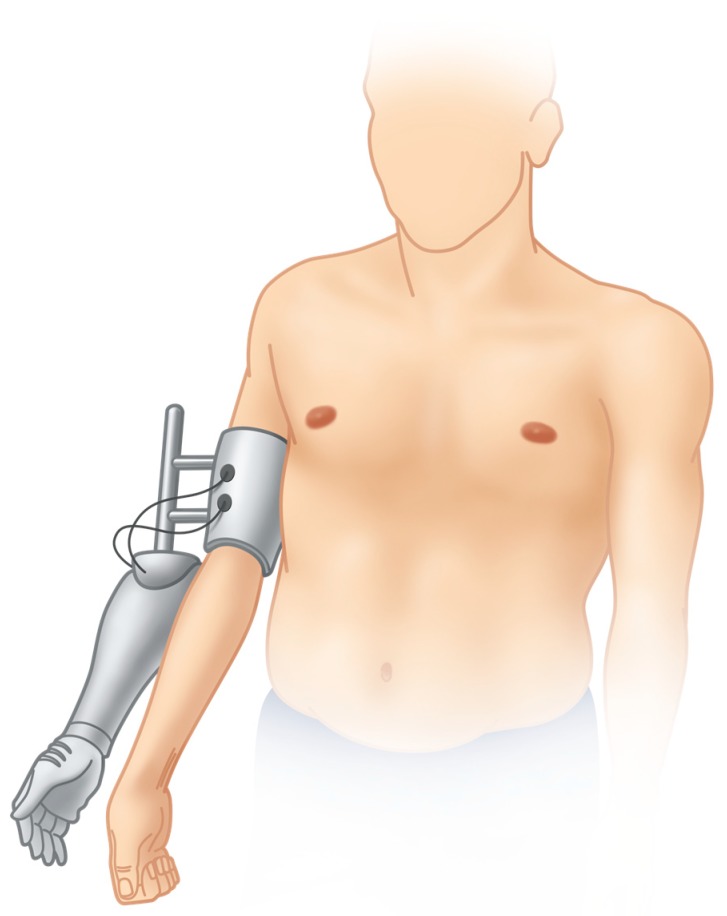
Global brachial plexopathies including multiple nerve root avulsions may result in complete upper limb paralysis despite surgical treatment. Bionic reconstruction, which includes the elective amputation of the functionless hand and its replacement with a mechatronic device, has been described for the transradial level. Here, we present for the first time that patients with global brachial plexus avulsion injuries and lack of biological shoulder and elbow function benefit from above-elbow amputation and prosthetic rehabilitation. Between 2012 and 2017, forty-five patients with global brachial plexus injuries approached our centre, of which nineteen (42.2%) were treated with bionic reconstruction. While fourteen patients were amputated at the transradial level, the entire upper limb was replaced with a prosthetic arm in a total of five patients. Global upper extremity function before and after bionic arm substitution was assessed using two objective hand function tests, the action research arm test (ARAT), and the Southampton hand assessment procedure (SHAP). Other outcome measures included the DASH questionnaire, VAS to assess deafferentation pain and the SF-36 health survey to evaluate changes in quality of life. Using a hybrid prosthetic arm mean ARAT scores improved from 0.6 ± 1.3 to 11.0 ± 6.7 (p = 0.042) and mean SHAP scores increased from 4.0 ± 3.7 to 13.8 ± 9.2 (p = 0.058). After prosthetic arm replacement mean DASH scores improved from 52.5 ± 9.4 to 31.2 ± 9.8 (p = 0.003). Deafferentation pain decreased from mean VAS 8.5 ± 1.0 to 6.7 ± 2.1 (p = 0.055), while the physical and mental component summary scale as part of the SF-36 health survey improved from 32.9 ± 6.4 to 40.4 ± 9.4 (p = 0.058) and 43.6 ± 8.9 to 57.3 ± 5.5 (p = 0.021), respectively. Bionic reconstruction can restore simple but robust arm and hand function in longstanding brachial plexus patients with lack of treatment alternatives.
Keywords: artificial limbs; bionics; brachial plexus injury; chronic pain; nerve root avulsion; prostheses and implants; prosthesis fitting.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Algorithm for bionic hand reconstruction in patients with global brachial plexopathies.J Neurosurg. 2017 Nov;127(5):1163-1171. doi: 10.3171/2016.6.JNS16154. Epub 2017 Jan 17. J Neurosurg. 2017. PMID: 28093018
-
The Vienna psychosocial assessment procedure for bionic reconstruction in patients with global brachial plexus injuries.PLoS One. 2018 Jan 3;13(1):e0189592. doi: 10.1371/journal.pone.0189592. eCollection 2018. PLoS One. 2018. PMID: 29298304 Free PMC article.
-
Bionic reconstruction to restore hand function after brachial plexus injury: a case series of three patients.Lancet. 2015 May 30;385(9983):2183-9. doi: 10.1016/S0140-6736(14)61776-1. Epub 2015 Feb 25. Lancet. 2015. PMID: 25724529
-
[Prosthetic reconstruction of the upper extremity].Unfallchirurg. 2016 May;119(5):408-13. doi: 10.1007/s00113-016-0174-4. Unfallchirurg. 2016. PMID: 27160727 Review. German.
-
[Nerve transfer (neurotization) for functional reconstruction of arm functions in cervical root avulsions].Orthopade. 1997 Jul;26(7):606-11. doi: 10.1007/s001320050130. Orthopade. 1997. PMID: 9340589 Review. German.
Cited by
-
[Prosthetic Fitting Concepts after Major Amputation in the Upper Limb - an Overview of Current Possibilities].Handchir Mikrochir Plast Chir. 2024 Feb;56(1):84-92. doi: 10.1055/a-2260-9842. Epub 2024 Feb 28. Handchir Mikrochir Plast Chir. 2024. PMID: 38417811 Free PMC article. German.
-
A BIONIC HAND VS. A REPLANTED HAND.J Rehabil Med Clin Commun. 2024 Jan 18;7:24854. doi: 10.2340/jrmcc.v7.24854. eCollection 2024. J Rehabil Med Clin Commun. 2024. PMID: 38274357 Free PMC article.
-
Bionic Prostheses: The Emerging Alternative to Vascularised Composite Allotransplantation of the Limb.Front Surg. 2022 May 6;9:873507. doi: 10.3389/fsurg.2022.873507. eCollection 2022. Front Surg. 2022. PMID: 35599802 Free PMC article. Review.
-
Outcome Measures Used to Assess Hand Activity in Amputee and Intact Populations: a Literature Review.Can Prosthet Orthot J. 2022 Dec 25;5(2):39023. doi: 10.33137/cpoj.v5i2.39023. eCollection 2022. Can Prosthet Orthot J. 2022. PMID: 37614636 Free PMC article. Review.
-
Brachial Plexus Injuries in Sport Medicine: Clinical Evaluation, Diagnostic Approaches, Treatment Options, and Rehabilitative Interventions.J Funct Morphol Kinesiol. 2020 Mar 30;5(2):22. doi: 10.3390/jfmk5020022. J Funct Morphol Kinesiol. 2020. PMID: 33467238 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
