

Pathologists' agreement on treatment suggestions for melanocytic skin lesions
- PMID: 31862403
- PMCID: PMC8824529
- DOI: 10.1016/j.jaad.2019.12.020
Pathologists' agreement on treatment suggestions for melanocytic skin lesions
Abstract
Background: Although treatment guidelines exist for melanoma in situ and invasive melanoma, guidelines for other melanocytic skin lesions do not exist.
Objective: To examine pathologists' treatment suggestions for a broad spectrum of melanocytic skin lesions and compare them with existing guidelines.
Methods: Pathologists (N = 187) completed a survey and then provided diagnoses and treatment suggestions for 240 melanocytic skin lesions. Physician characteristics associated with treatment suggestions were evaluated with multivariable modeling.
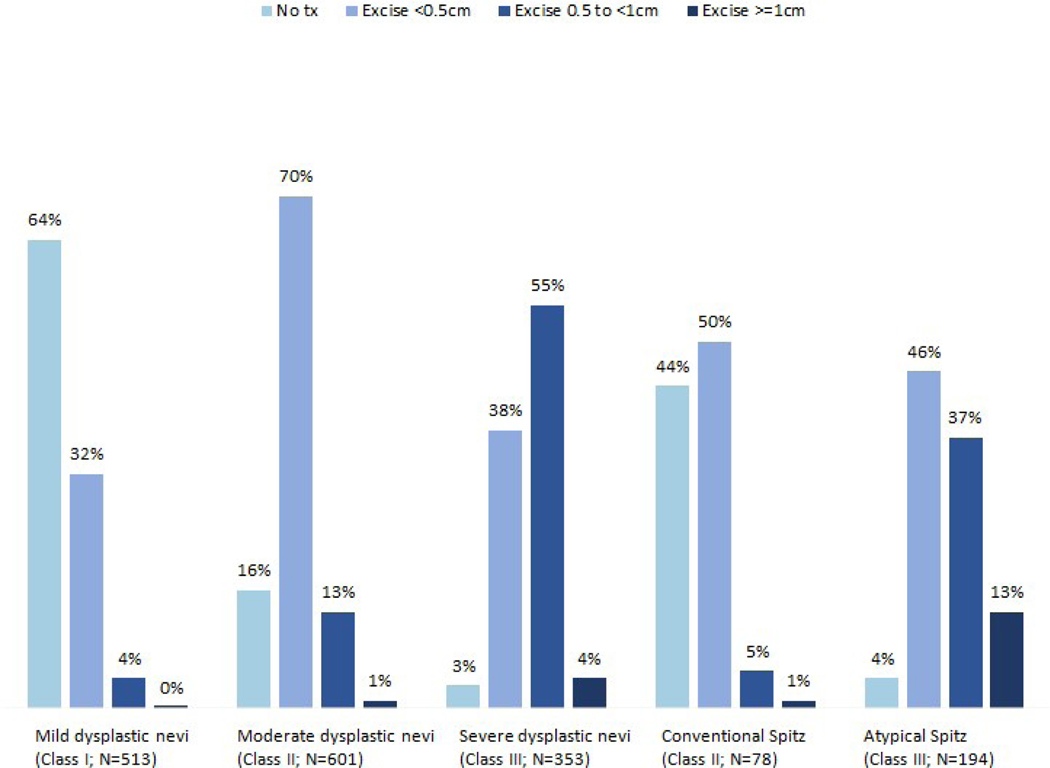
Results: Treatment suggestions were concordant with National Comprehensive Cancer Network guidelines for the majority of cases interpreted as melanoma in situ (73%) and invasive melanoma (86%). Greater variability of treatment suggestions was seen for other lesion types without existing treatment guidelines. Characteristics associated with provision of treatment suggestions discordant with National Comprehensive Cancer Network guidelines were low caseloads (invasive melanoma), lack of fellowship training or board certification (melanoma in situ), and more than 10 years of experience (invasive melanoma and melanoma in situ).
Limitations: Pathologists could not perform immunohistochemical staining or other diagnostic tests; only 1 glass side was provided per biopsy case.
Conclusions: Pathologists' treatment suggestions vary significantly for melanocytic lesions, with lower variability for lesion types with national guidelines. Results suggest the need for standardization of treatment guidelines for all melanocytic lesion types.
Keywords: invasive melanoma; melanocytic skin lesions; melanoma in situ; pathology; skin biopsies; treatment guidelines.
Copyright © 2019 American Academy of Dermatology, Inc. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Similar articles
-
Variation among pathologists' treatment suggestions for melanocytic lesions: A survey of pathologists.J Am Acad Dermatol. 2017 Jan;76(1):121-128. doi: 10.1016/j.jaad.2016.07.029. Epub 2016 Sep 28. J Am Acad Dermatol. 2017. PMID: 27692732 Free PMC article.
-
Pathologist characteristics associated with accuracy and reproducibility of melanocytic skin lesion interpretation.J Am Acad Dermatol. 2018 Jul;79(1):52-59.e5. doi: 10.1016/j.jaad.2018.02.070. Epub 2018 Mar 7. J Am Acad Dermatol. 2018. PMID: 29524584 Free PMC article.
-
Pathologist Characteristics Associated With Rendering Higher-Grade Diagnoses for Melanocytic Lesions.JAMA Dermatol. 2023 Dec 1;159(12):1315-1322. doi: 10.1001/jamadermatol.2023.4334. JAMA Dermatol. 2023. PMID: 37938821 Free PMC article.
-
Role of In Vivo Reflectance Confocal Microscopy in the Analysis of Melanocytic Lesions.Acta Dermatovenerol Croat. 2018 Apr;26(1):64-67. Acta Dermatovenerol Croat. 2018. PMID: 29782304 Review.
-
Common and not so Common Melanocytic Lesions in Children and Adolescents.Pediatr Dev Pathol. 2018 Mar-Apr;21(2):252-270. doi: 10.1177/1093526617751720. Pediatr Dev Pathol. 2018. PMID: 29607755 Review.
Cited by
-
The potential of x-ray virtual histology in the diagnosis of skin tumors.Skin Res Technol. 2024 Oct;30(10):e13801. doi: 10.1111/srt.13801. Skin Res Technol. 2024. PMID: 39363439 Free PMC article.
-
Unveiling documentation deficiencies: a clinical audit of histopathology request forms at a tertiary care hospital.Ann Med Surg (Lond). 2025 Mar 27;87(4):2000-2005. doi: 10.1097/MS9.0000000000003038. eCollection 2025 Apr. Ann Med Surg (Lond). 2025. PMID: 40212126 Free PMC article.
-
Diagnostic error, uncertainty, and overdiagnosis in melanoma.Pathology. 2023 Mar;55(2):206-213. doi: 10.1016/j.pathol.2022.12.345. Epub 2022 Dec 29. Pathology. 2023. PMID: 36642569 Free PMC article. Review.
References
-
- Hocker TL, Alikhan A, Comfere NI, Peters MS. Favorable long-term outcomes in patients with histologically dysplastic nevi that approach a specimen border. J Am Acad Dermatol. 2013;68(4):545–551. - PubMed
-
- Fleming NH, Egbert BM, Kim J, Swetter SM. Reexamining the Threshold for Reexcision of Histologically Transected Dysplastic Nevi. JAMA Dermatol. 2016;152(12):1327–1334. - PubMed
-
- Engeln K, Peters K, Ho J, et al. Dysplastic nevi with severe atypia: Long-term outcomes in patients with and without re-excision. J Am Acad Dermatol. 2017;76(2):244–249. - PubMed
