

A case of lupus vasculopathy presenting favorable renal outcome
- PMID: 31863345
- PMCID: PMC6990287
- DOI: 10.1007/s13730-019-00431-2
A case of lupus vasculopathy presenting favorable renal outcome
Abstract
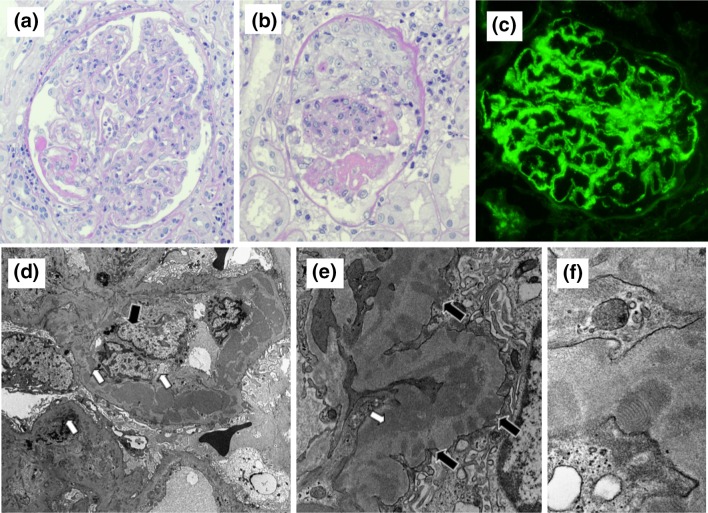
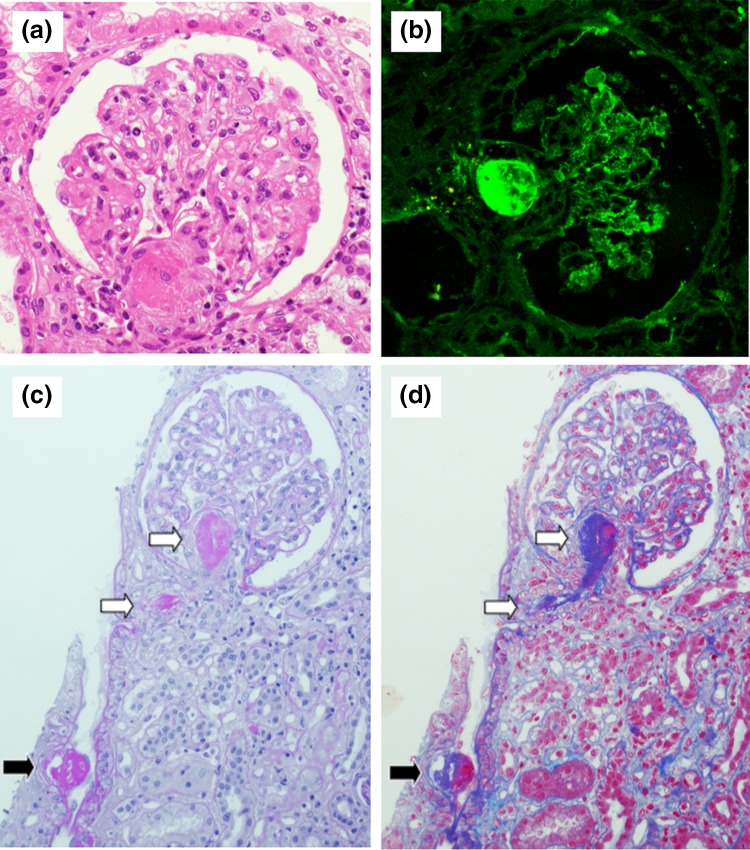
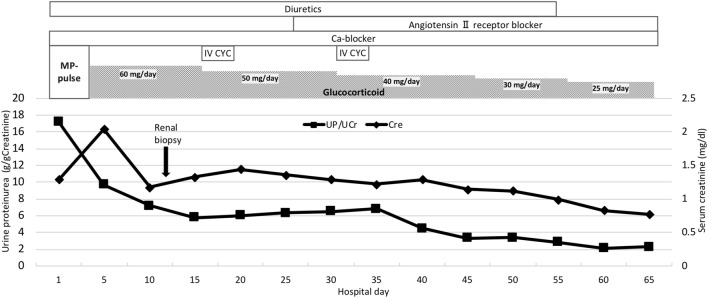
Noninflammatory necrotizing vasculopathy, also referred to as lupus vasculopathy, is not infrequently observed in the pathology of lupus nephritis. It affects vessels causing them to become severely narrowed and occluded by a mechanism involving immune complexes. We experienced a 51-year-old woman with lupus nephritis class IV + V, which was accompanied by lupus vasculopathy. Renal biopsy and light microscopy showed eosinophilic hyaline-like material in the afferent and/or efferent arterioles, which narrowed the lumen, and which were positive for IgG by immunofluorescent analysis. Electron microscopy indicated that amorphous material and endothelial detachment occluded the arterioles. These findings were consistent with those of lupus vasculopathy. We treated the patient with steroids and cyclophosphamide. By the day of discharge, her levels of creatinine and proteinuria had undergone partial remission. Although lupus vasculopathy was implied as a lesion with unfavorable renal prognosis, some recent reports suggest its true renal prognosis is not unfavorable necessarily. Nevertheless, lupus vasculopathy is an important finding in diagnosis in contradiction to other vascular legions in systemic lupus erythematosus. In addition, a standard therapy has also not been established. Therefore, it is important to accumulate cases of lupus vasculopathy to determine its prognosis and develop standard treatments.
Keywords: Lupus nephritis; Lupus vasculopathy; Noninflammatory necrotizing vasculopathy.
Conflict of interest statement
The authors have declared that no conflict of interest exists.
Figures
References
-
- Klemperer P, Pollack AD, Baehr G. Pathology of disseminated lupus erythematous. Arch Pathol. 1941;32:569–631.
-
- Appel GB, Pirani CL, D’Agati V. Renal vascular complications of systemic lupus erythematosus. J Am Soc Nephrol. 1994;4(8):1499–1515. - PubMed
-
- Banfi G, Bertani T, Boeri V, Faraggiana T, Mazzucco G, Monga G, et al. Renal vascular lesions as a marker of poor prognosis in patients with lupus nephritis: Gruppo Italiano per lo Studio della Nefrite Lupica (GISNEL) Am J Kidney Dis. 1991;18(2):240–248. doi: 10.1016/S0272-6386(12)80885-7. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
