

Comparison of biparametric and multiparametric MRI in the diagnosis of prostate cancer
- PMID: 31864408
- PMCID: PMC6925429
- DOI: 10.1186/s40644-019-0274-9
Comparison of biparametric and multiparametric MRI in the diagnosis of prostate cancer
Abstract
Purpose: To compare the diagnostic accuracy of biparametric MRI (bpMRI) and multiparametric MRI (mpMRI) for prostate cancer (PCa) and clinically significant prostate cancer (csPCa) and to explore the application value of dynamic contrast-enhanced (DCE) MRI in prostate imaging.
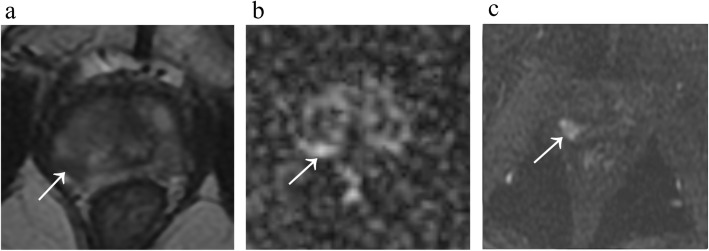
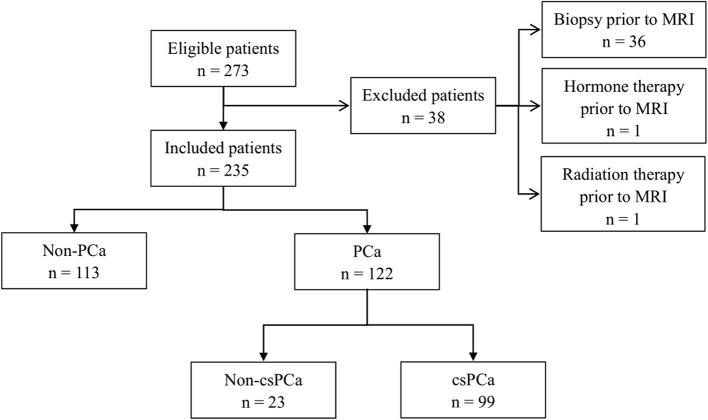
Methods and materials: This study retrospectively enrolled 235 patients with suspected PCa in our hospital from January 2016 to December 2017, and all lesions were histopathologically confirmed. The lesions were scored according to the Prostate Imaging Reporting and Data System version 2 (PI-RADS V2). The bpMRI (T2-weighted imaging [T2WI], diffusion-weighted imaging [DWI]/apparent diffusion coefficient [ADC]) and mpMRI (T2WI, DWI/ADC and DCE) scores were recorded to plot the receiver operating characteristic (ROC) curves. The area under the curve (AUC), accuracy, sensitivity, specificity, negative predictive value (NPV), and positive predictive value (PPV) for each method were calculated and compared. The patients were further stratified according to bpMRI scores (bpMRI ≥3, and bpMRI = 3, 4, 5) to analyse the difference in DCE MRI between PCa and non-PCa lesions (as well as between csPCa and non-csPCa).
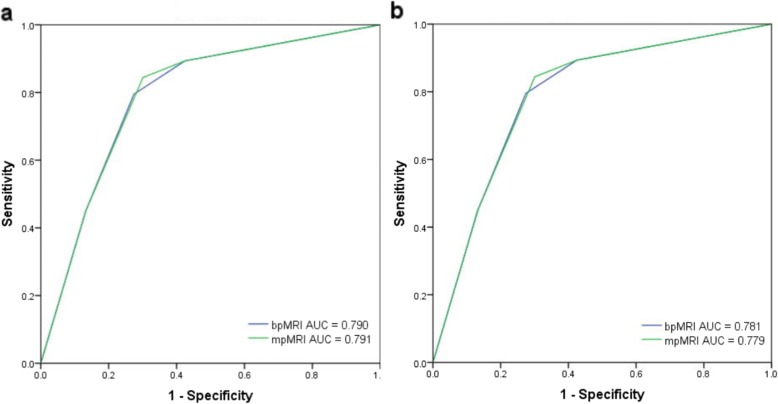
Results: The AUC values for the bpMRI and mpMRI protocols for PCa were comparable (0.790 [0.732-0.840] and 0.791 [0.733-0.841], respectively). The accuracy, sensitivity, specificity, PPV and NPV of bpMRI for PCa were 76.2, 79.5, 72.6, 75.8, and 76.6%, respectively, and the values for mpMRI were 77.4, 84.4, 69.9, 75.2, and 80.6%, respectively. The AUC values for the bpMRI and mpMRI protocols for the diagnosis of csPCa were similar (0.781 [0.722-0.832] and 0.779 [0.721-0.831], respectively). The accuracy, sensitivity, specificity, PPV and NPV of bpMRI for csPCa were 74.0, 83.8, 66.9, 64.8, and 85.0%, respectively; and 73.6, 87.9, 63.2, 63.2, and 87.8%, respectively, for mpMRI. For patients with bpMRI scores ≥3, positive DCE results were more common in PCa and csPCa lesions (both P = 0.001). Further stratification analysis showed that for patients with a bpMRI score = 4, PCa and csPCa lesions were more likely to have positive DCE results (P = 0.003 and P < 0.001, respectively).
Conclusion: The diagnostic accuracy of bpMRI is comparable with that of mpMRI in the detection of PCa and the identification of csPCa. DCE MRI is helpful in further identifying PCa and csPCa lesions in patients with bpMRI ≥3, especially bpMRI = 4, which may be conducive to achieving a more accurate PCa risk stratification. Rather than omitting DCE, we think further comprehensive studies are required for prostate MRI.
Keywords: Dynamic contrasted-enhanced imaging; Magnetic resonance imaging; Prostate cancer; Prostate imaging reporting and data system.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- 7192176/Beijing Municipal Natural Science Foundation
- 3332018022/Fundamental Research Funds for the Central Universities
- 10023201700104/Education Reform Fund of Peking Union Medical College
- 91859119/National Natural Science Foundation of China
- No. 2019PT320008 and 2018PT32003/National Public Welfare Basic Scientific Research Project of Chinese Academy of Medical Sciences
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
