

The socioeconomic burden of chronic lung disease in low-resource settings across the globe - an observational FRESH AIR study
- PMID: 31864411
- PMCID: PMC6925865
- DOI: 10.1186/s12931-019-1255-z
The socioeconomic burden of chronic lung disease in low-resource settings across the globe - an observational FRESH AIR study
Abstract
Background: Low-resource settings are disproportionally burdened by chronic lung disease due to early childhood disadvantages and indoor/outdoor air pollution. However, data on the socioeconomic impact of respiratory diseases in these settings are largely lacking. Therefore, we aimed to estimate the chronic lung disease-related socioeconomic burden in diverse low-resource settings across the globe. To inform governmental and health policy, we focused on work productivity and activity impairment and its modifiable clinical and environmental risk factors.
Methods: We performed a cross-sectional, observational FRESH AIR study in Uganda, Vietnam, Kyrgyzstan, and Greece. We assessed the chronic lung disease-related socioeconomic burden using validated questionnaires among spirometry-diagnosed COPD and/or asthma patients (total N = 1040). Predictors for a higher burden were studied using multivariable linear regression models including demographics (e.g. age, gender), health parameters (breathlessness, comorbidities), and risk factors for chronic lung disease (smoking, solid fuel use). We applied identical models per country, which we subsequently meta-analyzed.
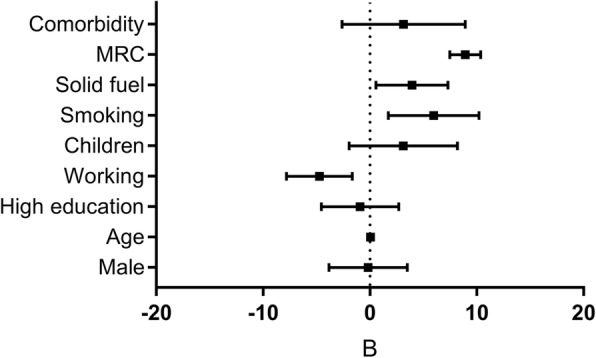
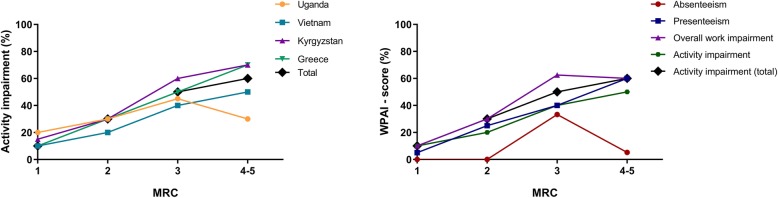
Results: Employed patients reported a median [IQR] overall work impairment due to chronic lung disease of 30% [1.8-51.7] and decreased productivity (presenteeism) of 20.0% [0.0-40.0]. Remarkably, work time missed (absenteeism) was 0.0% [0.0-16.7]. The total population reported 40.0% [20.0-60.0] impairment in daily activities. Breathlessness severity (MRC-scale) (B = 8.92, 95%CI = 7.47-10.36), smoking (B = 5.97, 95%CI = 1.73-10.22), and solid fuel use (B = 3.94, 95%CI = 0.56-7.31) were potentially modifiable risk factors for impairment.
Conclusions: In low-resource settings, chronic lung disease-related absenteeism is relatively low compared to the substantial presenteeism and activity impairment. Possibly, given the lack of social security systems, relatively few people take days off work at the expense of decreased productivity. Breathlessness (MRC-score), smoking, and solid fuel use are potentially modifiable predictors for higher impairment. Results warrant increased awareness, preventive actions and clinical management of lung diseases in low-resource settings from health policymakers and healthcare workers.
Keywords: Chronic lung disease; Chronic respiratory disease; Health economics; Household air pollution; Low-income population; Low-resource countries; Obstructive lung disease; WPAI; Work.
Conflict of interest statement
None to declare. Part of the results of this study have been previously reported in preliminary form as an abstract [51].
Figures



References
-
- World Health Organization. Chronic respiratory diseases. 2018. http://www.who.int/respiratory/en/. Accessed 8 Oct 2019.
-
- World Health Organization. Global Surveillance, prevention and control of chronic respiratory diseases: a comprehensive approach. 2007. http://www.who.int/gard/publications/GARD%20Book%202007.pdf. Accessed 7 Oct 2019.
-
- Beran D, Zar HJ, Perrin C, Menezes AM, Burney P, Forum of international respiratory societies working group c Burden of asthma and chronic obstructive pulmonary disease and access to essential medicines in low-income and middle-income countries. Lancet Respir Med. 2015;3:159–170. doi: 10.1016/S2213-2600(15)00004-1. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
