

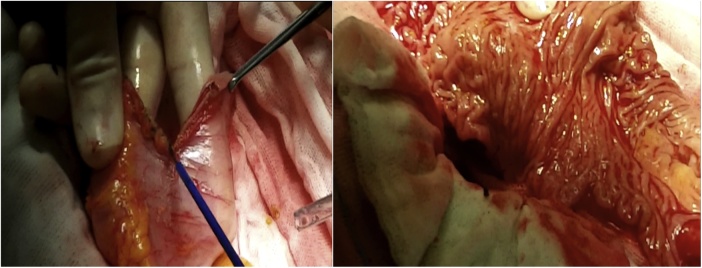
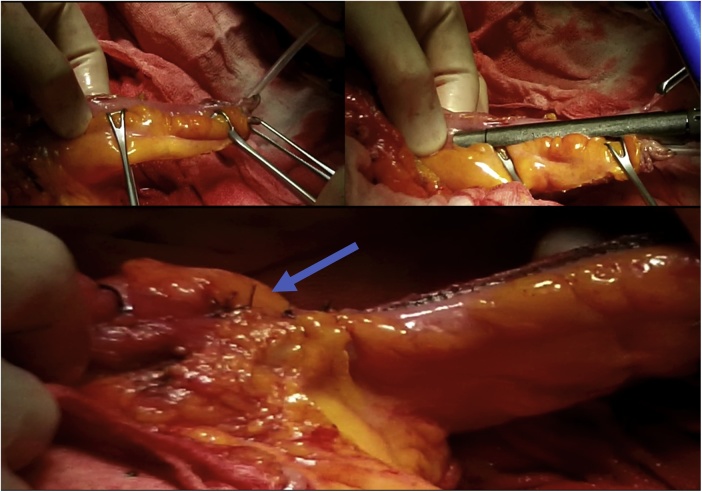
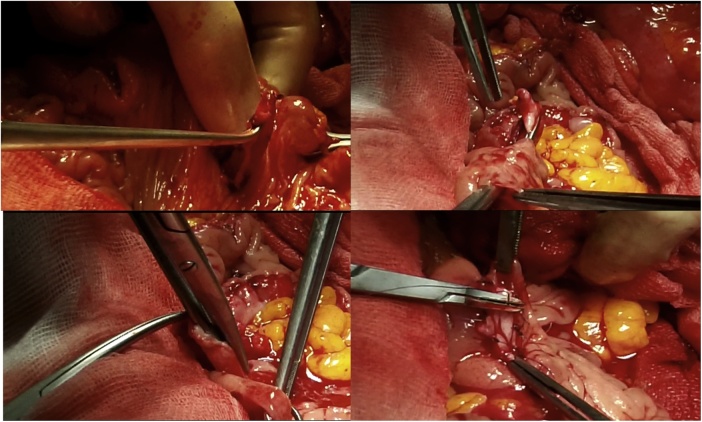
Step by step Indiana pouch construction in a previously irradiated patient with a cervical cancer relapse
- PMID: 31865230
- PMCID: PMC6928324
- DOI: 10.1016/j.ijscr.2019.11.068
Step by step Indiana pouch construction in a previously irradiated patient with a cervical cancer relapse
Abstract
Introduction: Radiation therapy and radical pelvic surgery, either radical cystectomy or pelvic exenteration, is the golden standard treatment for infiltrating bladder carcinoma, as well as advanced or recurrent cervical, vulvar, vaginal and endometrial cancer. However, due to the poor radiation sensitivity of the cervix and vagina, a high-radiation dose is required, leading to early and/or late onset urogenital complications in approximately 50% of the patients.
Case presentation: The following case report describes a 64-year-old native Russian woman presenting a relapse of a vaginal cuff squamous cell carcinoma, who underwent a laterally extended endopelvic resection (LEER) followed by a neobladder reconstruction based on the Indiana pouch (IP) technique. The process is described here step by step.
Discussion: Indiana pouch urinary diversion was based on thorough research, the reproducibility of the technique, our urologist's experience with the Indiana Pouch, as well the lower rate of complications published in various separate series.
Conclusion: Indiana pouch is a successful continence urinary reservoir with a reproductible technique, however long-term observation is needed.
Keywords: Cervical cancer; Indiana Pouch (IP); LEER; Previously irradiated pelvis; Step by step.
Copyright © 2019 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors declare no conflict of interest.
Figures








References
-
- Jordan G.H., Schellhammer P.F. AUA Update Series VI: 2-7. 1987. Complications after pelvic irradiation of urologic and gynecologic malignancy. - PubMed
-
- Eifel P.J., Levenback C., Wharton J.T. Time course and incidence of late complications in patients treated with radiation therapy for FIGO stage IB carcinoma of the uterine cervix. Int. J. Radiat. Oncol. Biol. Phys. 1995;32:1289–1300. - PubMed
-
- Leissner J. Colon Pouch (Mainz Pouch III) for continent urinary diversion after pelvic irradiation. Urology. 2000;56(5):798–802. - PubMed
-
- Wilkin Michael. Long-term complications associated with the indiana pouch urinary diversion in patients with recurrent gynecologic cancers after high-dose radiation. Urol. Oncol. 2005;23(1):12–15. - PubMed
-
- Bricker Eugene M. Bladder substitution after pelvic evisceration. J. Urol. 2002;167(2):1140–1145. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
