

Hypophysitis: An update on the novel forms, diagnosis and management of disorders of pituitary inflammation
- PMID: 31866206
- PMCID: PMC7078033
- DOI: 10.1016/j.beem.2019.101371
Hypophysitis: An update on the novel forms, diagnosis and management of disorders of pituitary inflammation
Abstract
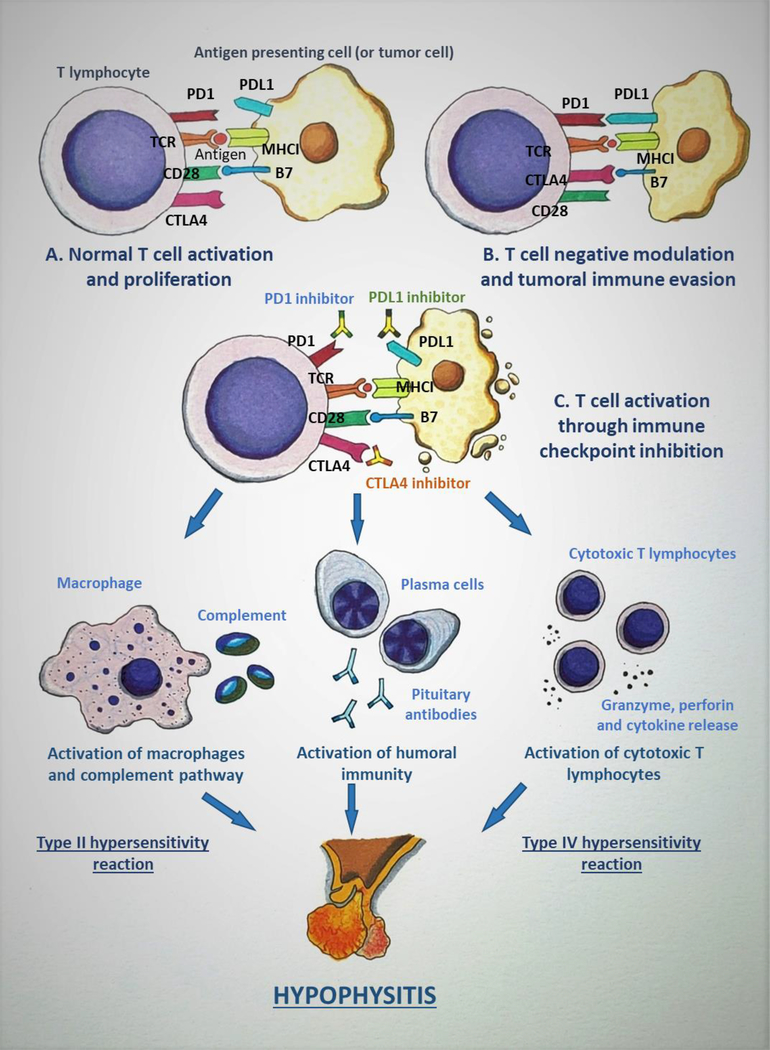
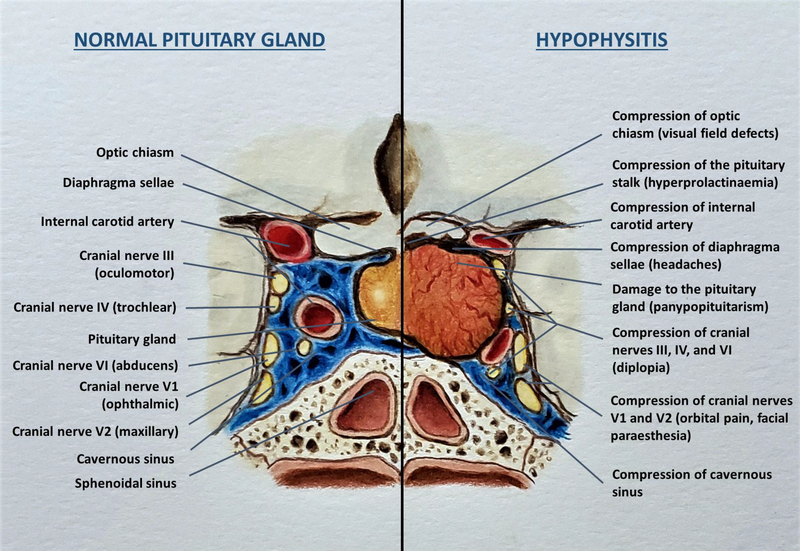
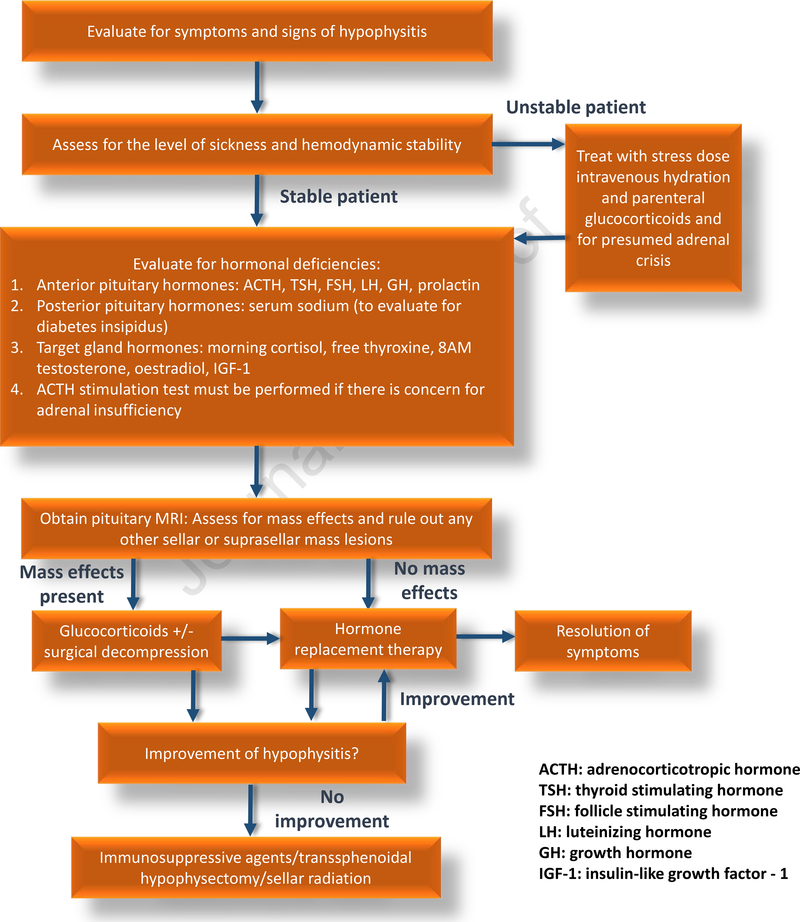
Hypophysitis is a heterogeneous condition that leads to inflammation of the sella and/or suprasellar region, potentially resulting in hormonal deficiencies and/or mass effects. A preponderance of hypophysitis subtypes have an underlying autoimmune aetiology. The overall incidence and prevalence of hypophysitis has dramatically increased over the past decade, mainly due to increased awareness of the condition in the medical community, improvements in imaging techniques, and a rise in the occurrence of certain forms of hypophysitis such as IgG4 hypophysitis (IgG4Hy) and immune checkpoint inhibitor induced hypophysitis (ICIHy). The clinical presentation varies from an asymptomatic condition to a fatal disease often as a result of electrolyte abnormalities due to glucocorticoid deficiency in the context of adrenal crisis from central adrenal insufficiency. Milder forms of hypophysitis are treated with replacement of deficient hormones while more acute presentations with mass effects require glucocorticoid therapy, immunosuppressive therapy or surgery. Timely diagnosis and interventions are keys to prevention of the lethal complications of this disease. In this review, we provide an update on the recent advances in the field of pituitary autoimmunity, with an emphasis on autoimmune hypophysitis and novel forms of hypophysitis such as anti-PIT1 hypophysitis, IgG4Hy and ICIHy.
Keywords: adrenal insufficiency; autoimmunity; hypophysitis; immune checkpoint inhibitors; immunotherapy; pituitary.
Published by Elsevier Ltd.
Conflict of interest statement
Declaration of Competing Interest This research was supported in part by the Intramural Research Program of the NIDDK and Eunice Kennedy Shriver NICHD, National Institutes of Health, Bethesda, MD.
Figures
References
-
- Wehbeh L, Alreddawi S, Salvatori R. Hypophysitis in the era of immune checkpoint inhibitors and immunoglobulin G4-related disease. Expert review of endocrinology & metabolism. 2019;14(3):167–78. - PubMed
-
- Koch CA, Antonelli A. Immunoendocrinology: When (neuro) endocrinology and immunology meet. Reviews in Endocrine and Metabolic Disorders. 2018;19(4):277–82. - PubMed
-
- Falorni A, Minarelli V, Bartoloni E, Alunno A, Gerli R. Diagnosis and classification of autoimmune hypophysitis. Autoimmunity Reviews. 2014;13(4–5):412–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
