Clinical features and treatment outcomes of opportunistic infections among human T-lymphotrophic virus type 1 (HTLV-1) carriers and patients with adult T-cell leukemia-lymphoma (ATL) at a single institution from 2006 to 2016
- PMID: 31866618
- PMCID: PMC6954174
- DOI: 10.3960/jslrt.18032
Clinical features and treatment outcomes of opportunistic infections among human T-lymphotrophic virus type 1 (HTLV-1) carriers and patients with adult T-cell leukemia-lymphoma (ATL) at a single institution from 2006 to 2016
Abstract
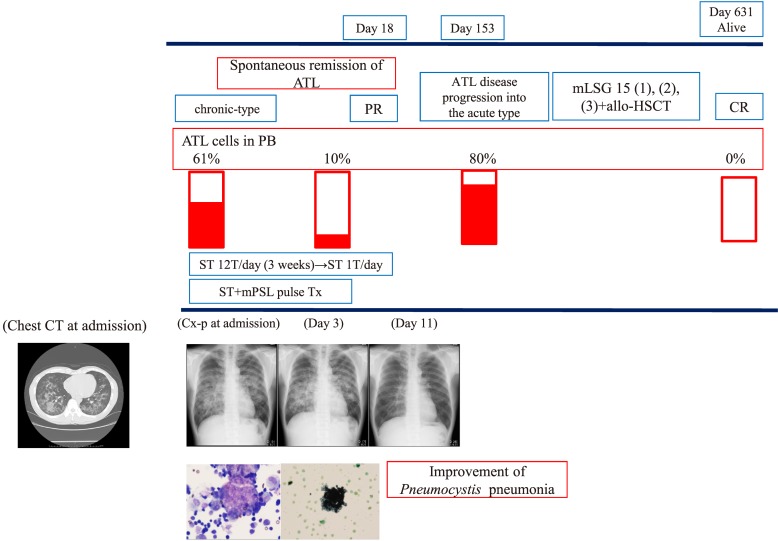
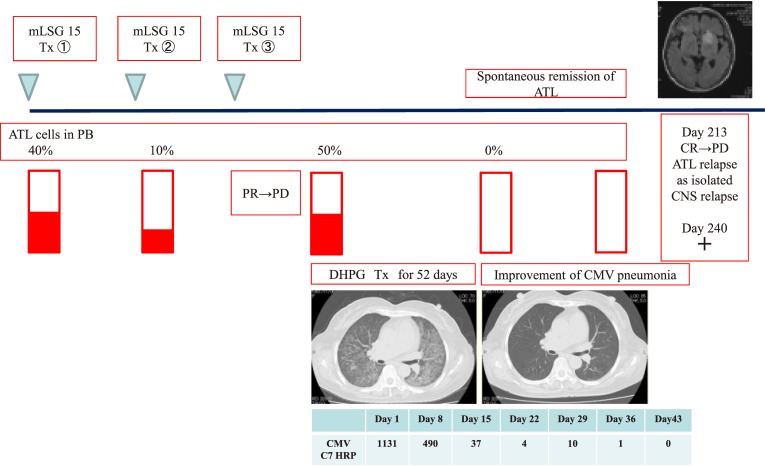
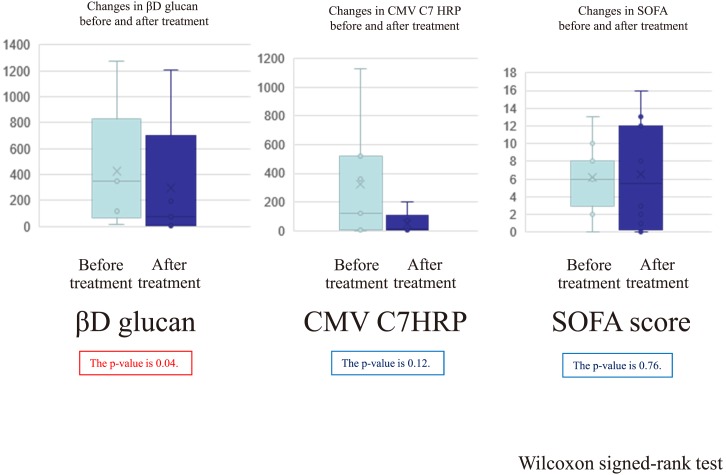
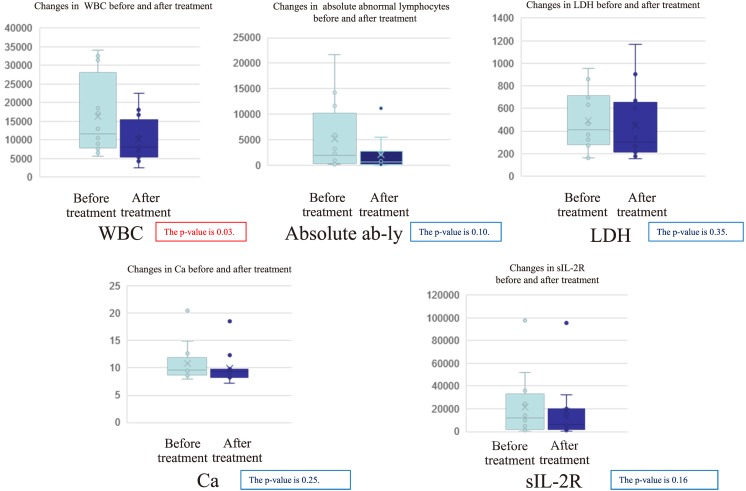
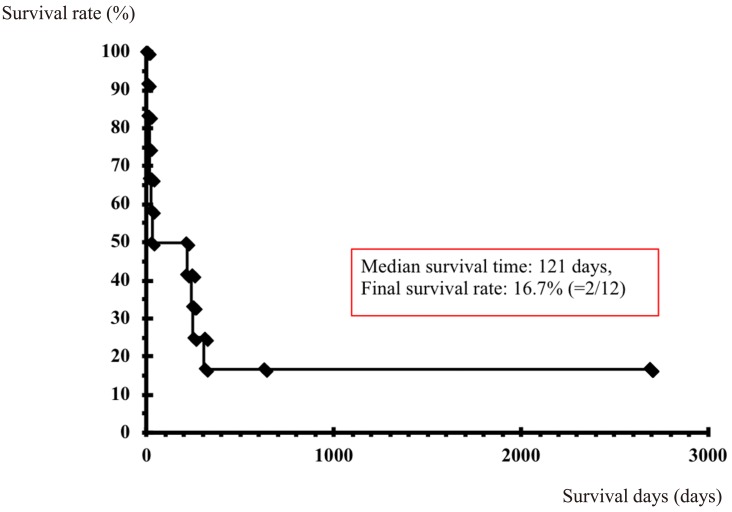
As opportunistic infections among human T-lymphotrophic virus type 1 (HTLV-1) carriers and patients with adult T-cell leukemia/lymphoma (ATL) pose a serious problem, it is necessary to clarify their clinical characteristics and outcomes in these patients. We retrospectively analyzed the clinical features and outcomes of opportunistic infections in 127 HTLV-1 carriers and 153 ATL patients between 2006 and 2016. The cumulative incidence rates of opportunistic infections among HTLV-1 carriers and ATL patients were 1.5% (2/127) and 6.5% (10/153), respectively. The etiology of opportunistic infections was as follows: fungal infections (3 cases), pneumocystis pneumonia, and cytomegalovirus (CMV) infections. Even after aggressive treatment, the prognosis of opportunistic infections was poor (50% of overall survival at 28 days). Regarding prognostic factors affecting the OS of opportunistic infections, higher SOFA scores (especially the respiratory subscore) and higher LDH values were identified by univariate analysis. Moreover, 3 out of 6 patients achieved spontaneous remission of ATL as the short-term outcome after the development of opportunistic infection. However, 5 out of 6 surviving patients exhibited ATL progression or relapse after a median of 194 days (133-226) after contracting an opportunistic infection as the long-term outcome of ATL. In conclusion, opportunistic infections should be carefully followed among HTLV-1 carriers and ATL patients because of their aggressive clinical course and poor outcomes. Furthermore, early diagnosis and subsequent prompt treatment are necessary in clinical practice.
Keywords: HTLV-1 carrier; adult T-cell leukemia/lymphoma; opportunistic infection; progression of ATL; spontaneous remission of ATL.
Conflict of interest statement
Figures